Ischemia
What is Ischemia?
Ischemia is a clinical condition in which the blood flow to vital organs gets reduced or restricted. Depending on the organ, the condition may be called cardiac ischemia, kidney ischemia, or brain ischemia. In babies, when the blood does not adequately flow to the brain in the prenatal or neonatal stage, it is known as infant brain ischemia.

Blood is the carrier of oxygen and other essential nutrients to the brain cells. When the blood supply to the baby’s brain is interrupted, the oxygen deficiency can result in improper brain function leading to developmental delays. If the ischemic condition continues for long, the infant may suffer a birth injury resulting in permanent brain damage.
In the event of a complete obstruction or partial constriction of oxygenated blood flow that supports the metabolic processes in the brain, the baby experiences cerebral anoxia or hypoxia. When this occurs during the labor and delivery process, birth or shortly after birth (in the neonatal period) doctors and nurses have a short window of time within which they must act to restore the oxygen flow. Failing this, the baby will experience a cascade of ischemic events in the brain, which ultimately lead to cerebral tissue death. Additional damage to other vital organs, such as the heart, liver and kidneys may also occur in many cases.
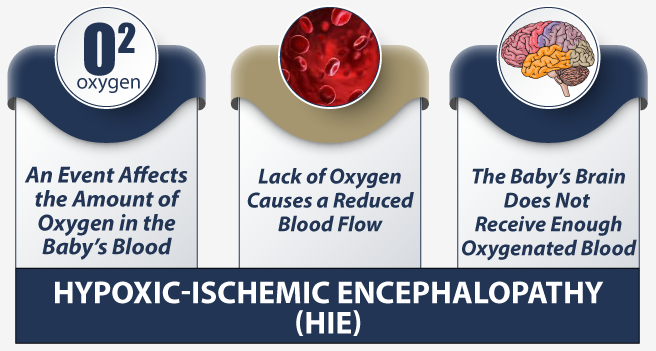
Hypoxic Ischemic Encephalopathy (HIE) and Hypoxia-Ischemia (HI) Injury
Infant brain ischemia, clinically known as neonatal hypoxia-ischemia (HI), is completely preventable in most cases. Neonatal HI injury is clinically defined as stoppage of the umbilical blood flow to the fetus at a gestational age of 36 weeks or above, including during the neonatal period after birth. Neonatal Ischemia continues to be the predominant cause of disability and death in infants, and is also commonly associated with lasting cognitive, sensory, and motor impairment in children including cerebral palsy.
When a baby suffers brain damage from ischemia prior to birth and shortly thereafter, the birth injury causes a brain condition known as hypoxic ischemic encephalopathy (HIE). The leading cause of cerebral palsy is HIE. Babies born with HIE have a high incidence of developmental delay and cognitive disability.
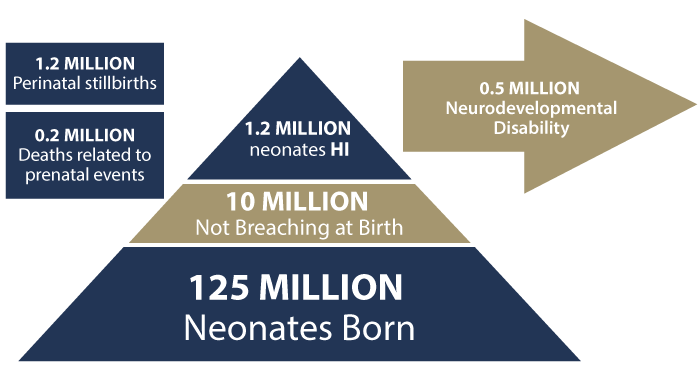
Neonatal HI is responsible for nearly one in four infant deaths worldwide. Children who survive the neonatal brain ischemic injury typically have a high rate of permanent disability. Research shows that among the infants who survived neonatal HI, up to 10% suffer from lasting motor disabilities, and up to 50% sustain cognitive or sensory deficits that continue to adolescence. A 7-study meta-analysis of 386 babies showed the following outcomes:
- 5.9% of the infants died
- 17.2% suffered neurological abnormalities
- 16.3% experienced neonatal seizures
- 14.2% qualified for a cerebral palsy diagnosis
Motor, sensory, and cognitive disorders resulting from infant brain ischemia include seizures, vision and hearing impairment, muscle spasticity, microcephaly (abnormally small head), language disorders, and learning disorders.
Signs and Symptoms of Infant Brain Ischemia
If a baby suffers an ischemic event prior to birth—during labor and delivery---the baby will have certain physiological responses that doctors (obstetricians), mid-wives and nurses can see that will enable them to respond to stop the ischemic event. These include:
- Fetal Distress
- Bradycardia
- Decelerations including recurrent late and variable
- Loss of Fetal Heart Rate variability
- Decreased fetal movement
- Abnormal Biophysical Profile
- Abnormal Nonstress Test
During an ischemic event after birth, as the infant’s brain begins to shut down because of oxygen starvation, various body organs start getting affected. Brain ischemia symptoms in babies can look similar to those suffering a stroke, and may include:
- Seizures
- Dizziness
- Loss of coordination
- Vertigo (inner ear and brain miscommunication)
- Vision or hearing impairment
- Feeble crying or no crying
- Fatigue and muscular lethargy
- Weakness in the entire body or certain body parts
- Loss of movement in the limbs
- Unconsciousness
Long-term Effects of Infant Brain Ischemia
Brief periods of ischemia (known as a transient ischemic attack) may cause temporary neurological symptoms in neonates. However, prolonged periods of ischemia can have more permanent effects.
Children who survive brain ischemia may experience serious disorders and development lapses (akin to an adult that survived a stroke) after the ischemic event is over. The actual impact will vary depending on the duration of ischemia and the area of the brain that suffered damage. Moreover, some of the following effects may start manifesting soon after birth:
- Epilepsy
- Traumatic brain injury
- Personality and mood disorders
- Lowered IQ
- Delays in the attainment of infant developmental milestones
- Cognitive impairment in comparison to peers
- Notable impairment of motor function
- Cerebral palsy
Types of Cerebral Ischemia causing Birth Injury and HIE
Researchers have classified infant cerebral ischemia into two categories, depending on the ischemia’s relative distribution. These include:
Focal Brain Ischemia
This occurs when a blood vessel in the brain gets blocked usually due to a blood clot. Focal brain ischemia restricts the blood flow to a specific area of the brain, leading to an increased risk of brain tissue death in that location. This type of cerebral ischemia may be caused because of the development of thrombosis (localized blood coagulation) or severe thromboembolic complications (when a piece of the blood clot breaks off and causes obstruction.)
Global Brain Ischemia
When the flow of oxygenated blood is temporarily restricted but restored quickly with medical resuscitation, it would be treated as transient ischemia. Symptoms in this case may last only briefly. If the oxygenation to the baby’s brain is not restored for a longer time period, it may result in a hypoxic state of global brain ischemia. This generally causes widespread damage to the white matter of the brain. If the ischemia so great that it results in complete restriction of the oxygen to the brain, an anoxic brain injury occurs usually resulting in damage to the grey matter of the brain.
In either case, the infant may suffer permanent brain damage or death. Reperfusion therapy and hypothermia therapy (“cooling”) may be instituted to preserve maximum brain tissue.
Hypothermia Therapy: The therapy involves cooling the baby’s core temperature to around 92.3 degrees Fahrenheit. After 72 hours, medical staff begin to gradually rewarm the baby while simultaneously monitoring the baby’s vital signs. Cooling or rewarming too quickly can harm the baby’s brain and other organs.
Reperfusion Therapy: a medical treatment to restore blood flow, either through or around, blocked arteries, typically after a heart attack (myocardial infarction (MI)). Reperfusion therapy includes drugs and surgery. The drugs are thrombolytics and fibrinolytics used in a process called thrombolysis.
What Causes Fetal and Infant Cerebral Ischemia?
According to the National Institutes of Health (NIH), cerebral ischemia injuries (including HIE) newborns often originate from fetal distress during labor leading to a birth injury, particularly when both baby and mother have a higher risk of complications. Other causes may range from viruses to hereditary factors to the mother’s lifestyle choices. A family history of compromised immune systems, neurological disorders, and congenital abnormalities may also contribute to a higher risk of infant brain ischemia.
Some of the known causes and risk factors of infant cerebral ischemia prior to and shortly after birth include:
- Oxygen deprivation during birth
- Uterine rupture including during a VBAC delivery
- Complications of the umbilical cord
- Placental abruptions
- Blood vessel compression during birth
- Preeclampsia (maternal high blood pressure)
- Infections, such as chickenpox or meningitis
- Prolonged or Arrested labor
- Blood clotting disorder in the infant and the mother
- Prolonged or distressed labor
- Preterm delivery before full in-utero lung development
- Congenital heart defect
- Neonatal Hypoglycemia
- Mistakes during Neonatal Resuscitation
- Failure to provide Hypothermia (“Cooling”) Therapy
- Meconium Aspiration Syndrome (MAS)
- Gestational diabetes
- Maternal hypotension causing insufficiency of infant brain oxygenation
The extent of lasting infant brain damage during the period of oxygen deprivation will ultimately depend on the particular area of the brain that sustained the maximum cellular deterioration and death of the neurons following the anoxic condition.
Diagnostic Tests to Determine Infant Brain Ischemia
In a suspected case of infant brain ischemia, the medical providers will usually require a series of tests to scan the brain for tumors, lesions, or other signs that indicate an ischemic condition. Other body parts may also be evaluated to check for potential abnormalities.
The diagnostic criteria for infant hypoxia ischemia are generally based on the following set of markers:
- APGAR Scores: The 5-minute Apgar score is usually below 5. But not all APGAR scores are correctly calculated or recorded
- Whether the baby requires neonatal resuscitation including intubation to provide mechanical ventilation and CPR.
- Metabolic Acidosis from arterial blood gases drawn from the baby at birth
- Absence of sucking reflex, hypotonic muscles, or other abnormal neurological indicators
- Abnormal MRI findings prior to any hypothermia therapy
Structural Imaging Tests to Evaluate the Baby’s Neuroanatomy for HIE from Ischemia
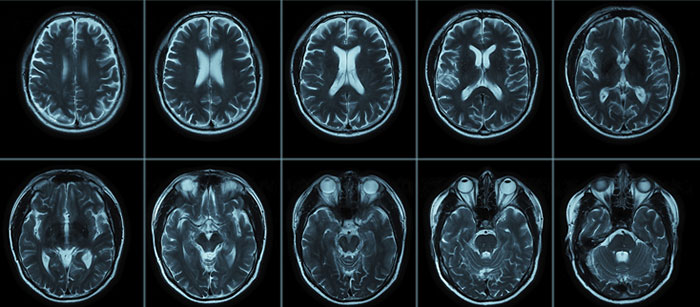
Structural imaging tests can show cerebral damage (HIE) that has occurred prior to, at or shortly after birth in newborns that survive the initial hypoxic-ischemic insult. Magnetic Resonance Imaging (MRI) test will usually detect injury to the:
- Thalamus: part of the brain that relays the motor and sensory signals to the brain
- Basal ganglia: brain nuclei responsible for motor control, executive functions, and emotions
- Cerebral cortex: the “grey matter” involved in complex brain functions, such as information processing and language ability
- White Matter: is the surface area of the brain and damage can result when ischemia is due to prolonged hypoxia vs. a sudden (acute) and complete restriction of the blood flow.
In other words, there is no single region of the brain that might suffer specific damage due to an ischemic event.
MRI
To investigate the neonatal brain anatomy, diffusion-weighted MRI imaging (DWI) may be a more reliable technique. It can determine the time of the brain lesion onset. (DWI can sensitively measure the mobility of water molecules in the brain tissue, known as Brownian movement.)
Changes in the basal ganglia lesions in the first few days after birth can be detected with sequential MRI imaging. If the white matter diffusion in the brain appears asymmetric from the scan, it may be correlated with severe hemiparesis (partial paralysis or muscle weakness in one side of the body.)
Other Diagnostic Tools
Electroencephalography (EEG) has been shown to be a reliable predictor of neonatal HIE clinical outcomes. In particular, aEEG or amplitude-integrated EEG is a more effective technique. A vital EEG measure of neurodevelopment in infants is the Thompson score (or the HIE score). This measure comprises clinical symptoms associated with the dysfunction of the central nervous system (CNS). It helps assess the newborn’s status after birth asphyxia.
In the Thompson scoring system, 0 is considered the normal score, while 22 is the worst score, signifying most severe hypoxic ischemic encephalopathy (HIE) status.
Cranial ultrasound and magnetic resonance spectroscopy (MRS) are other useful clinical tools that help in understanding infant brain ischemia. MRS technique allows the real time imaging of the brain metabolism to identify processes that may be inhibiting brain activity.
How do the Brain Cells Die During Infant Brain Ischemia?
Following moderate or severe brain ischemia, the loss of brain tissue (brain cell death) in babies primarily occurs due to three pathways:
- Inflammation: Encephalitis resulting from viral infection or other causes
- Oxidative stress: A chemical process that results in the production of free radicals following a lack of oxygen supply to the brain
- Excitotoxicity: A phenomenon causing nerve cell death following pathologically high levels of glutamate (causing neurotoxicity)
Neonatal brain ischemia and hypoxic ischemic injury in babies is fundamentally different from the ischemic stroke seen in adults. A severe ischemic event in a baby’s brain (either before or shortly after birth) may cause a dissolution of the brain’s outermost basal tissue layer due to cell death. This may occur because the newly developed blood vessels in infants are fragile and are highly vulnerable to rupture. This is the not the case after an adult stroke.
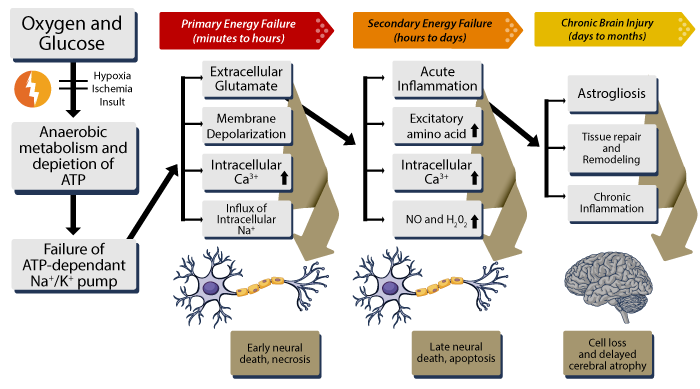
Ischemic Injury May Occur in Phases
Injuries related to infant brain ischemia may evolve over time as follows:
- Primary phase: In the first few hours following the brain ischemic event, the MRI scan may detect only a subtle injury (restricted diffusion that starts as tiny lesions in the thalami and putamen.) Over the next three to four days, it tends to spread to more extensive regions of the brain.
- Secondary phase: In the days following the baby’s brain ischemic injury, a secondary injury phase may develop. This could lead to loss of cerebral autoregulation, MOMP or mitochondrial permeabilization (release of mitochondrial proteins that lead to death of brain cells), and neuroinflammation (inflammation of the nervous tissue).
- Tertiary phase: Following a hypoxic ischemic insult in the baby, active pathological processes of the brain may continue to take place for weeks, months or even years. This may cause persistent inflammatory damage and epigenetic changes (changes in the genetic makeup resulting from persistent behavioral changes).
Male babies are at a Greater Risk of HIE and Cerebral Palsy
Cohort studies have shown that near-term or full-term male babies are more vulnerable to ischemic or hypoxic-ischemic injury compared to females. Brain repair after an ischemic stroke in male infants is also relatively limited, contributing to a higher incidence of poor cognitive and motor outcomes in comparison to female infants with a similar injury.
Quantitative imaging results also reveal that preterm male infants are at a higher risk of white matter injury (white matter is found in the sub-cortical or deeper brain tissue, and is responsible for information transfer). On the other hand, preterm female infants are more prone to grey matter injury (grey matter is composed of the neuronal cells in the brain, responsible for speech, hearing, vision, emotions, decision making, and muscle control.)
Researchers are currently unable to explain the causes behind these sexual dimorphic outcomes in males and females as a consequence of infant brain ischemia. But this does not mean only male babies can suffer a birth injury leading to HIE or cerebral palsy. A female baby can suffer from fetal distress or any other event that leads to ischemia and also suffer a serious HIE injury resulting in lifelong complications even cerebral palsy.
Treatments for Infant Brain Ischemia
Treatment modalities will depend on the child’s age, severity of symptoms, and the underlying causes of the ischemic event and/or the ongoing condition. If the baby experiences seizures, the medical provider may prescribe anticonvulsant drugs to stop or limit their frequency.
Therapeutic hypothermia is currently used as one of the more effective, non-invasive treatments for infant brain ischemia. Hypothermia involves cooling the newborn’s body at a temperature of about 91.4°F for a continuous period of 72 hours. Research has shown that this treatment may mitigate the brain damage and the resulting neurological impairments, including fatality rates in the affected infants.
Stemming from this, therapeutic hypothermia alone may not suffice to prevent or reduce the effects of infant brain ischemia. The medical team must consider additional therapies that could be used in conjunction with it to achieve better outcomes.
Later in life babies suffering from an ischemic brain injury may receive physical therapy and occupational therapy. Occupational therapy teaches the child how to adapt to their condition and become independent as far as possible.
Additional strategies to address complications from an ischemic birth injury may include behavioral therapy, speech therapy, use of assistive devices, treatment for hearing or vision impairments, and educational interventions.
Treatments for Arterial Ischemic Stroke in Neonates
Arterial ischemic stroke is the most common form of neonatal stroke (or pediatric stroke). This may occur when the blood flow to the infant’s brain or spinal cord is obstructed due to a structural abnormality or a blood clot. Treatments in the early stages of the neonatal stroke can support the restoration of blood supply to the brain. The following treatments may be considered independently or as a combination:
Medical Therapy
The child may be administered anticoagulants (blood thinners) along with special vitamin supplements. Transfusion therapy or hydroxurea medication therapy may be given individually or in combination to the child. Anti-seizure drugs may be added to the therapy if the child is experiencing seizures. Clot removal drugs which are prescribed for adults are not approved for use in babies, but the medical team may consider this option in specific circumstances.
Interventional Neuroradiology
This treatment may be considered if the child has aneurysm (the blood vessel walls are weakened, causing them to bulge and burst) or arteriovenous malformation (abnormalities in blood vessels delivering oxygen to the brain). To repair the abnormal vessels, the medical provider will insert a catheter through the leg or arm, and guide it into the affected blood vessels in the brain.
Brain Surgery
In specific cases of pediatric stroke or certain other cerebrovascular disorders, a surgical procedure may be recommended. If the child suffers from severe swelling in the brain, a craniectomy may be performed to remove a portion of the bone. Other surgeries for pediatric stroke include removal of abnormal tissue in the brain, closure of abnormal blood vessels, or rerouting of blood vessels to feed the brain’s injured areas.
Is Your Child’s Brain Ischemia Birth Injury the Result of Medical Malpractice?
Parents whose children suffer from a birth injury causing brain ischemia deserve an answer to how their child developed this condition and whether it was preventable. Our dedicated birth injury lawyers want to help you find those answers.
If your child has been diagnosed with infant brain ischemia or HIE, and you suspect this may have been caused in part by medical mistakes, Miller Weisbrod Olesky will thoroughly investigate the facts and hold responsible medical providers accountable by pursuing medical malpractice claims against them. The compensation our clients receive helps them pay for their child’s current and future medical treatment, therapy, equipment needed to help cope with disabilities, and the other expenses associated with caring for a child with brain injuries, seizure disorders, organ damage, speech, vision, hearing or motor impairments, and cerebral palsy.
Sometimes families are hesitant to reach out to a medical malpractice attorney or law firm. Other parents feel overwhelmed by their circumstances and worried that they will not be able to help out in a lawsuit involving their child’s birth injury.
Miller Weisbrod Olesky is different from most law firms.
We provide help NOW.
Many attorneys focus only on pursuing their client’s legal case. At Miller Weisbrod Olesky, we know your child needs help today – not just when your birth injury lawsuit is settled. We have a team focused on helping our clients NOW when they need it most.

We know that children with birth injuries like hypoxic-ischemic encephalopathy (HIE) and cerebral palsy often require intense therapy, specialized medical treatment, and assistive care. The stress of providing for a birth injured child’s needs can be both emotionally and financially draining.
But just ‘knowing’ this is not enough. We act on this knowledge by providing exceptional services to birth-injured children and their families.
While Miller Weisbrod Olesky’s birth injury attorneys aggressively prepare each legal case, another department goes into action to help the families of children we represent. Led by a nurse-attorney, this department acts as a medical case manager for our birth injury clients by:
- Regularly monitoring the child’s medical treatment status,
- Helping facilitate medical treatment and therapy, and
- Arranging transportation and services.
Where necessary, we also help families locate local medical providers specializing in the care and treatment of children who have suffered a birth injury. With Miller Weisbrod Olesky, you’re not just a ‘case’. And that’s important when you’re looking for a lawyer who can help you cope with your child’s needs today.
Please call or email us today to get started.
Registered Nurses and Nurse-Attorneys Are a Vital Part of Our Birth Injury Team … and Yours

Most national birth injury law firms will employ one or two nurses to assist the review of cases and medical research. But Miller Weisbrod Olesky offers an unmatched number of nurses and nurse-attorney employees support to both the birth injury attorneys and our clients.
Our team of registered nursing staff and nurse-attorneys bring a deep level of medical and personal insight to every client’s case. Our nursing team includes both an experienced labor and delivery nurse as well as an ICU nurse. Working closely with the rest of the team, they investigate the reasons behind a birth injury and how medical professionals breached their standard of care.
Why Should You Talk with the Knowledgeable Attorneys at Miller Weisbrod Olesky?

The only way to find out if you have a birth injury case is to talk to a medical negligence attorney who understands how ischemia occurs during labor and delivery, birth and shortly after birth if baby’s are not correctly monitored, diagnosed and treated.
At Miller Weisbrod Olesky, a team of committed attorneys, nurses and paraprofessionals uses our detailed medical negligence case review process to assess your potential claim. We start by learning more about you and your child and the status of meeting/missing developmental milestones. Then we gather medical records to determine what happened before, during, and after your delivery. We call in skilled medical experts who review your records and let us know if they think medical errors could have caused your child’s injuries.
If we feel medical negligence caused or contributed to your child’s injuries, we meet with you to discuss how you can receive compensation from the medical professionals who made the errors.
At no point in our legal intake process will we ask you to pay anything. The medical review of your case and the consultation are free. We only receive payment when you do.
Contact Our National Birth Injury Lawyers
National Birth Injury Law
Our National Birth Injury Attorneys, nurses, and support staff understand that parents of children with birth injuries feel overwhelmed. So, every client has the attention and support of a team of trained, compassionate professionals. But we don’t just offer compassion.
We offer a process to help you discover whether your child’s birth injury, HIE, cerebral palsy or brain injury at birth was caused by medical malpractice.
Call our offices today at (888) 987-0005 for experienced assistance in a free consultation.
Quick Links
Testimonials
- Lyric C. I feel like our voice was heard in a sense of what can possibly go wrong in a delivery and finding us answers. I feel with our settlement, we are now in a comfortable position to provide for our son.
- Lyssa L. They are not just people that say “hey let's get you money and let's go” The law firm was very thorough with us. It was awesome. I don't want to cry, because I think about and it's amazing that they were able to help me and that we were able to help my son and get the story out there.
- Jay C. Throughout the process, one thing was clear to us, the ultimate interest of our child was the utmost concern of Max and his team and as parents navigating a situation like that, that was refreshing to know we had them firmly on our side. I highly recommend them.
Popular Cities
- ★ Dallas Birth Injury
- ★ Houston Birth Injury
- ★ Atlanta Birth Injury
- ★ Chicago Birth Injury
- ★ Philadelphia Birth Injury
Locations
★ Dallas
11551 Forest Central Drive, Ste. 300
Dallas, TX 75243
★ Houston
12929 Gulf Freeway, Ste. 111
Houston, TX 77034