Neonatal Seizures
What are Neonatal Seizures?
Neonatal convulsions or neonatal seizures are epileptic fits that may occur during the first four weeks after birth (which is called the neonatal period). The first week after birth is particularly the most vulnerable for developing seizures.
Seizures during this time are often an important indicator that fetal distress and oxygen deprivation during the labor and delivery process. Newborn babies that suffer neonatal seizures are at high risk of other brain injuries such as hypoxic-ischemic encephalopathy (HIE) and cerebral palsy.

Neonatal seizures are the result of abnormal electrical activity in the brain usually caused by damage or injury to one or more areas of the brain. Neonatal seizures may only last for a few minutes, hours or days, but these short-lived events usually indicate major damage to the newborn’s brain or another serious brain malfunction. This condition should be treated as a neurological emergency, and the medical team must act fast to correctly diagnose and manage the condition.
Neonatal seizures are often a sign that the baby suffered fetal distress or birth trauma during the labor and delivery process or shortly after birth. When newborn (“neonatal”) seizures occur while the baby is still in the hospital shortly after birth, the medical providers must act quickly not only to control the seizures which can cause further brain damage due to oxygen deprivation (hypoxia/anoxia), but also determine if the cause of the seizures was a birth injury.
What Causes of Neonatal Seizures?
- Birth Trauma—including injury from compressive injuries, trauma induced strokes or fractures
- Birth injury including from hypoxia or anoxia as a result of fetal distress
- Hypoxic Ischemic Encephalopathy
- Infection
- Genetic abnormalities
- Metabolic disorders including metabolic acidosis
- Medications given during labor and delivery or shortly after birth
- Fever
Noteworthy Definitions:
- Neonatal Period: The first 28 days from the date of birth of a full-term infant
- Full-term Infant: The infant that has completed the gestational age of 40 weeks
- Gestational Age: The total duration of the pregnancy
- Chronological Age: The infant’s legal age from the date of birth
- Conceptional Age: The total of gestational age and chronological age
It is important that doctors (including neonatologists and pediatricians) and newborn and neonatal ICU nurses understand the different types of seizures and the signs of each type of seizure.
What are Types Neonatal Seizures?
Just like any other seizures, neonatal seizures are stereotypical, repetitive, and paroxysmal events. Five primary types of neonatal seizures include:
- Subtle seizures (50%)
- Clonic seizures (25%)
- Myoclonic seizures (20%)
- Tonic seizures (5%)
- Repetitive non-paroxysmal behaviors

Subtle Seizures
This is the most commonly type of neonatal seizure. As the name suggests, the clinical manifestations of these seizures are subtle and often overlooked. They are similar to normal reactions and behaviors, and may include:
- Eye movements, ranging from roving and random ocular movements to sustained upward deviation of the eyes, with/without jerking
- Fluttering or blinking eyelid, eye opening, rolling up the eyes, nystagmus, or gaze fixation
- Lingual, buccal, oral movements, such as tongue protrusions, chewing, smacking, and sucking
- Progression movements, such as struggling, thrashing, bicycling, pedaling, swimming, or rowing movements
- Purposeless complex movements, such as sudden episodes of limb hyperactivity & crying
Clonic Seizures
These motor seizures are marked by rhythmic jerks, which might be localized to a specific area of the limbs or face, the diaphragm and axial muscles (mid-section), or be hemi-convulsive (one side of the body) or multifocal (coming from different parts of the injured brain).
Myoclonic Seizures
These motor seizures are single, rapid, or repetitive arrhythmic jerks, affecting a limb, finger, or the entire body. They are seen more often in pre-term infants, which usually indicate a poor prognosis and a severe brain injury.
Tonic Seizures
These seizures will manifest with continuous muscle contraction in the axial, limb, facial, or other muscles. They could be asymmetrical or symmetrical, generalized, focal, or multifocal.
Infantile Spasms
These muscle spasms marked by short jerking spells of extension or flexion are relatively rare. They are quicker than tonic seizures, but slower in comparison to myoclonic seizures.
Hypoxic-Ischemic Encephalopathy (HIE)
A Key Cause of Neonatal Seizures and Epilepsy
Hypoxic-ischemic encephalopathy or HIE is recognized as one of the leading causes of neurological disorders, such as seizures/epilepsy, mental delay and cerebral palsy. Neonatal seizures could be an acute HIE consequence, which could result in further damage to the newborn’s brain.
HIE is a serious brain disorder that may develop due to lack of blood flow or oxygen to the brain for a certain time period. “Hypoxic” means insufficient oxygen; “ischemic” indicates insufficient blood flow; and “encephalopathy” refers to brain dysfunction.
HIE may occur at any stage – pregnancy, labor or delivery, or during the postnatal phase. While some children may only experience moderate health effects from HIE, others may suffer far more serious effects, such as epilepsy, motor impairment (cerebral palsy), cognitive impairment, developmental delays, and such other permanent and severe disabilities.
When the supply of oxygenated blood to the brain is disrupted, it may result in oxygen starvation of the rest of the body as well. The consequences could be damage to the liver, heart, bowels, kidneys, or other organs. When the brain suffers damage or injury in this condition, a full recovery may not occur. The severity of brain damage is correlated to the time period for which the oxygen supply was interrupted.
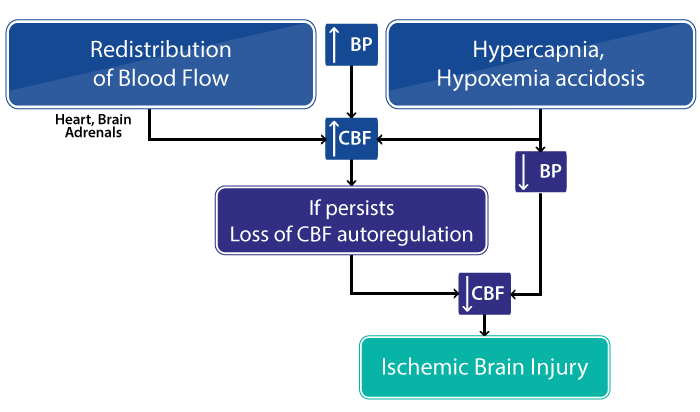
How does HIE Cause Neonatal Seizures?
The occurrence of HIE triggers a cascade of events which reduce the energy generation activity in the brain due to oxygen deprivation. This can result in neonatal seizures and overstimulation of the brain impulses. The hypoxic-ischemic event can be caused by multiple events, but ultimately brain injury occurs because of impaired cerebral blood flow (CBF) and oxygen delivery to the brain.
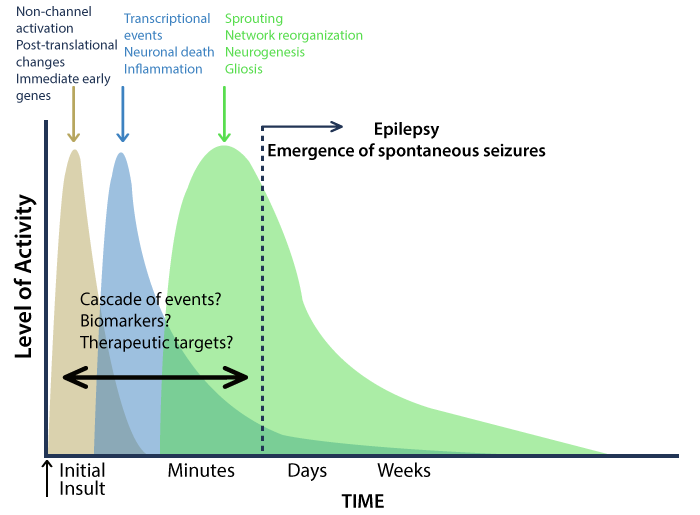
Oxygen deprivation or asphyxia also causes cellular damage, but the exact mechanism of how this damage occurs is still a matter of research. What is clear is that a series of neurochemical (nerve tissue chemical process) and inflammatory changes occur with asphyxia, resulting in the death of nerve cells.
HIE accounts for nearly 50 percent of neonatal seizures in both premature and full-term babies. Newborns with HIE often have a high seizure burden, which may result in status epilepticus in up to 15% of cases. (Status epilepticus is a life-threatening brain disease causing impairment of the respiratory function and airway control. It is marked by rapid or continuous seizure activity lasting for over 30 minutes – without recovery between episodes.)
Types of Seizures Caused by HIE
In four out of five cases, neonatal seizures are marked by unilateral, large infarcts (tissue death resulting from lack of oxygen supply). Seizures are often focal (partial) and contra-lateral (on the opposite side) to the cortical lesion (lesion on the external cerebrum layer).About two-thirds of the cases reveal cerebral venous infarcts (infarcts of the cerebral vein). Newborns with diffuse or multiple lesions along with cerebral venous infarcts usually have migratory or multifocal (multi-location) seizures.
Clonic seizures are often observed in these cases. When the medical provider holds the limb with clonic rhythmic contractions, they can feel the limb movement. Clonic activity does not get suppressed with limb extension or flexion, as it would in jitteriness.
Diagnosing Neonatal Seizures
An electroencephalogram (EEG) test is the gold standard for diagnosing neonatal seizures. The EEG device records the brain’s electrical activity. If abnormalities in this activity are detected (measured between seizures), it could be indicative of neonatal seizures. Neuroimaging tests, such as computed tomography (CT) scan and magnetic resonance imaging (MRI) are also used to diagnose seizures or to identify their cause. Cranial ultrasound may be performed to rule out intracranial hemorrhage (brain bleeds).
Differential Diagnosis
Differential diagnosis (differentiating between two similar-looking conditions) for neonatal seizures should include:
- Identifying any unusual stereotypical or repetitive movement during the neonatal phase as it could represent a seizure.
- Noting the changes in autonomic functions, such as the heart rate or blood pressure, which could be indicative of seizure activity.
- Finding any inconsistency in the relationship between EEG-detected abnormal electrical activity and a clinical seizure.
Seizure Assessment
Neonatal seizure assessment should involve a review of family history of epilepsy or seizures, gestational diabetes, infections or drug use during pregnancy, condition of the baby at birth (was there metabolic acidosis or low APGARS), birth trauma or birth injury history or fetal distress during labor. This assessment may give clues to the seizure etiology (manner of causation).
Pathology Tests
These may include full blood examination, blood glucose level, serum electrolytes, arterial blood gas, blood cultures, and lumbar puncture (if infection risk is indicated).
Treatment of Neonate Seizures
Following the early management and diagnosis of neonatal seizures and their possible underlying causes, the medical team should evaluate the seizure severity and duration to determine whether the baby must be treated with antiepileptic drugs (AED).
The FDA-approved Phenobarbital drug is usually the first treatment of choice for neonatal seizures. The drug has been in use for several decades as a therapy for seizures and is also used to treat status epilepticus.
Phenobarbital is a sleep-inducing barbiturate (based on barbituric acid) used as an anticonvulsant (drug to reduce the severity of convulsions or epileptic seizures) in sub-hypnotic doses. Babies with liver or kidney dysfunction may not be administered Phenobarbital in standard doses because it could prove toxic for these organs.
If this AED therapy fails to work, alternative treatments with Pyridoxine (vitamin B6) and/or folic acid (vitamin B9) should be considered. The medical team should ensure close monitoring of the baby in case of AED therapy, considering the toxicity risks. The baby’s blood work should be taken, and kidney and liver tests should be performed, apart from the standard monitoring procedures.
Needing Better Neonatal Seizure Treatments
Neonatal seizures can result in lifelong epilepsy, severe motor and cognitive impairment, and even death. The condition is often treatment resistant, in part because the treatments available for newborns are not very different from the treatments used for older children and adults with seizures. Therapies have not really changed for decades.
A prospective study at Boston Children’s Hospital found that out of 426 infants admitted consecutively, about 64% had neonatal seizures that did not respond to the early AED therapy, 16% were diagnosed with status epilepticus, and 17% died in the neonatal ICU.
Epilepsy Treatments for Young Children
Phenobarbital
As one of the oldest anticonvulsant medications, it is most commonly prescribed for infants and toddlers with epilepsy. It may initially cause drowsiness, but over time children may develop tolerance to it.
Valproic Acid
It is used to treat epilepsy in children and various types of childhood seizure disorders. Weight gain is a common side effect, but in some cases liver damage may occur with this medication.
Phenytoin
It is used both as a daily anticonvulsant and as an IV treatment in the ER to stop an ongoing seizure. Side effects may include weakened bones, involuntary eye movements, and hirsutism, among others.
Carbamazepine
This drug is used most effectively as a therapy for partial seizure disorders. It works well for students because it rarely interferes with learning ability and does not cause drowsiness in most cases.
Topiramate
This medication is used as an adjunct therapy with other drugs to treat epilepsy in children. Side effects may include dizziness, appetite loss, fatigue, and a tingling sensation in the hands and feet.
Epilepsy Surgery for Young Children
In certain cases, surgery may be recommended for young children who are diagnosed with intractable (hard to control) epilepsy. Very young children experiencing frequent and severe seizures that hamper their development and quality of life could be candidates for surgery. Children with focal seizures usually respond better to surgery compared to those with multifocal seizures.
Surgical procedures used currently may include temporal lobe resection (removing a circumscribed part of the temporal lobe) or hemispherectomy (removing almost half portion of the brain). The risks of intractable epilepsy must be weight against the risks of surgery. Infants may have higher likelihood of improved development outcomes post-surgery, but they also have a higher mortality rate compared to older children.
Implanted Electrical Devices
One of the commonly used electrical devices (battery operated) for young children with epilepsy is the vagal nerve stimulator. It is designed to deliver electrical signals intermittently to the vagus nerve in a cyclical manner. The signals get transmitted to the brain and help in inhibiting seizures. The device is implanted under the collarbone, and is known to reduce the frequency of seizures for some patients. Implanted electrical devices are not meant to replace drug therapy, but should only be used an adjunct treatment.
Medical Negligence that Contribute to Infant Seizures
Some of the common errors made by doctors and nurses that can cause a birth injury leading to seizures include:
- Failure to diagnose and treat the mother’s condition like preeclampsia, gestational diabetes, or maternal infection
- Failure to provide proper prenatal care and treatments for labor and delivery
- Delayed diagnosis and treatment of preterm labor
- Failure to diagnose fetal macrosomia (an abnormally large sized baby)
- Failing to react to umbilical cord complications
- Placental abruption, placental previa
- Failure to react to prolonged labor
- Failure to perform a timely c-section or vaginal delivery when the baby is in distress
- Failure to intervene in a timely manner to abnormal readings on the fetal heart rate monitor
- Inappropriate use of obstetrical forceps or vacuum extractors during delivery, causing injuries to the brain
- Failure to appropriately and timely provide neonatal resuscitation to the baby
- Failure to recognize and timely treat neonatal hypoglycemia
Are Your Child’s Seizure’s the Result of Medical Malpractice?
Parents whose children suffer from neonatal seizures or epilepsy deserve an answer to how their child developed this condition and whether it was preventable. Our dedicated birth injury lawyers want to help you find those answers.
If your child has been diagnosed with neonatal seizures or epilepsy, and you suspect this may have been caused in part by medical mistakes, Miller Weisbrod Olesky will thoroughly investigate the facts and hold responsible medical providers accountable by pursuing medical malpractice claims against them. The compensation our clients receive helps them pay for their child’s current and future medical treatment, therapy, equipment needed to help cope with disabilities, and the other expenses associated with caring for a child with brain injuries, seizure disorders, and cerebral palsy.
Sometimes families are hesitant to reach out to a medical malpractice attorney or law firm. Other parents feel overwhelmed by their circumstances and worried that they will not be able to help out in a lawsuit involving their child’s birth injury.

Why Should You Talk with the Knowledgeable Attorneys at Miller Weisbrod Olesky?
The only way to find out if you have a birth injury case is to talk to an attorney who understands birth injuries leading to a delay or failure in developmental milestones.
At Miller Weisbrod Olesky, a team of committed attorneys, nurses and paraprofessionals uses our detailed medical negligence case review process to assess your potential claim. We start by learning more about you and your child and the status of meeting/missing developmental milestones. Then we gather medical records to determine what happened before, during, and after your delivery. We call in skilled medical experts who review your records and let us know if they think medical errors could have caused your child’s injuries.
If we feel medical negligence caused or contributed to your child’s injuries, we meet with you to discuss how you can receive compensation from the medical professionals who made the errors.
At no point in our legal intake process will we ask you to pay anything. The medical review of your case and the consultation are free. We only receive payment when you do.
Contact Our National Birth Injury Lawyers
National Birth Injury Law
Our National Birth Injury Attorneys, nurses, and support staff understand that parents of children with birth injuries feel overwhelmed. So, every client has the attention and support of a team of trained, compassionate professionals. But we don’t just offer compassion.
We offer a process to help you discover whether your child’s birth injury, HIE, cerebral palsy or brain injury at birth was caused by medical malpractice.
Call our offices today at (888) 987-0005 for experienced assistance in a free consultation.
Quick Links
Testimonials
- Lyric C. I feel like our voice was heard in a sense of what can possibly go wrong in a delivery and finding us answers. I feel with our settlement, we are now in a comfortable position to provide for our son.
- Lyssa L. They are not just people that say “hey let's get you money and let's go” The law firm was very thorough with us. It was awesome. I don't want to cry, because I think about and it's amazing that they were able to help me and that we were able to help my son and get the story out there.
- Jay C. Throughout the process, one thing was clear to us, the ultimate interest of our child was the utmost concern of Max and his team and as parents navigating a situation like that, that was refreshing to know we had them firmly on our side. I highly recommend them.
Popular Cities
- ★ Dallas Birth Injury
- ★ Houston Birth Injury
- ★ Atlanta Birth Injury
- ★ Chicago Birth Injury
- ★ Philadelphia Birth Injury
Locations
★ Dallas
11551 Forest Central Drive, Ste. 300
Dallas, TX 75243
★ Houston
12929 Gulf Freeway, Ste. 111
Houston, TX 77034