Fetal Heart Rate Monitoring
Fetal & Maternal Monitoring
Why Checking a Baby’s Heart Rate During Delivery is So Important
Doctors must monitor expecting mothers before birth during their prenatal testing visits. They also check on the baby’s wellbeing using ultrasounds and devices that check their heartbeat.

Fetal monitoring often becomes critical when labor and delivery begin. During labor, fetal heart rates can signal when the baby is in fetal distress from reduced oxygen and blood flow.
When fetal monitoring strips show signs of fetal distress, medical professionals must immediately intervene to prevent oxygen deprivation. Prolonged periods of reduced oxygenation and blood flow to the baby’s brain can cause irreversible brain damage at birth.
Parents may not always realize the role that improper fetal heart rate monitoring played in causing a child’s brain injury. When healthcare providers miss signs of fetal distress and delay critical treatment like emergency C-sections, the baby can permanently suffer. Families of children who suffer from preventable birth injuries may have a viable medical malpractice claim.
Birth Injury Malpractice Attorneys
Miller Weisbrod Olesky's top rated birth injury attorneys specialize in identifying when improper heart rate monitoring causes or worsens a child’s birth injuries. If your baby suffered from the effects of birth injury negligence, don’t hesitate to contact our firm. We can answer difficult legal and medical questions and investigate the facts on your behalf.
Free Legal Consultation
Birth Injury Lawyers
(888) 987-0005Our Birth Injury Lawyers are available to meet you in your home or the hospital.
Our vast network of medical experts and in-house nursing staff and nurse-attorneys gives us the edge over our competition. When we take your case, we assign you with an entire medical team. This team not only consists of attorneys but also nursing advocates and medical experts.
Your team is available to assist with any day-to-day treatment you or your child may need. This includes assistance with medical records, scheduling doctors’ appointments, providing transportation, and any other problems that may arise.
We offer all of this on a contingency fee basis. This means you will not pay any fees until after we win your case and secure a settlement. Miller Weisbrod Olesky’s unmatched track record of birth injury results sets us apart from other birth injury law firms.

Recent Birth Injury Settlement:
Birth Injury settlement against a hospital in which nurses and physicians failed to properly monitor the mother's blood pressure during delivery causing an HIE event resulting in neonatal seizures and cerebral palsy at birth. Our team of top-rated birth injury lawyers recovered $13,750,000 for the family to help with future medical expenses and developmental therapy.
The Significance of Fetal Heart Rates

The fetal heart rate does not just tell us how the baby’s heart is doing. It’s also a sign of their overall health status.
The average fetal heart rate ranges between 110 and 160 beats per minute. The heart rate may vary between five to twenty-five beats faster or slower per minute. This is normal and a sign that the baby is healthy.
Abnormal fetal heart rates often indicate conditions like oxygen deprivation, shock, or infection that could affect the fetal brain. Unless doctors and other medical staff intervene, the baby could suffer from a complete lack of oxygen (“birth asphyxia”). When asphyxia or prolonged hypoxia occurs, a baby can sustain severe injuries like HIE, metabolic acidosis, or cerebral palsy.
How Do You Read Fetal Monitoring Strips?
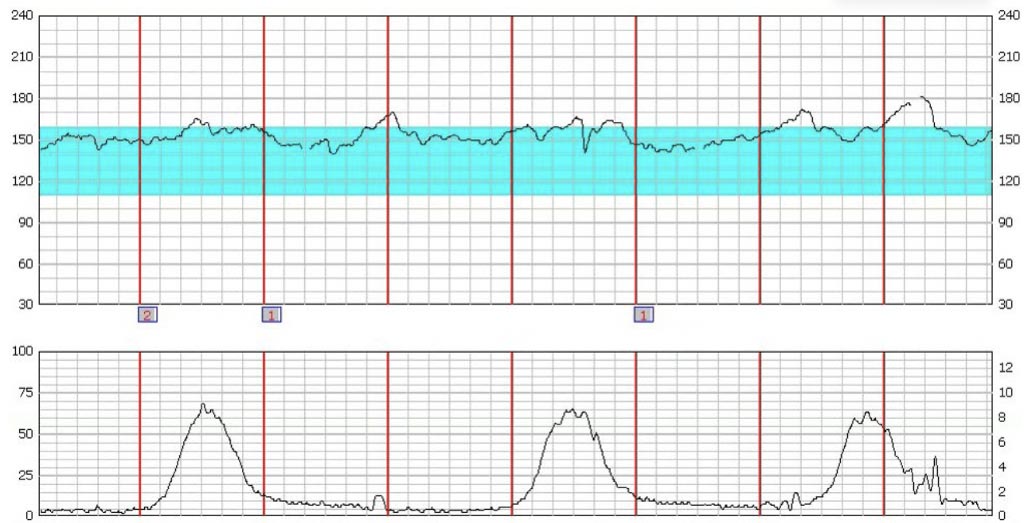
During labor, electronic fetal heart rate monitoring equipment carefully tracks the baby’s heart rate. The reading strip comes back in two pieces. The top part (highlighted in blue) measures the baby’s heart rate, and the bottom part measures the mother’s contractions. Each red line indicates one minute.
Why Monitor Fetal Heart Rates During Labor?

Doctors must closely monitor heart rates during labor due to the valuable insight they provide into the baby’s oxygen levels.
All fetal heart rates fluctuate during labor. Some changes are normal and not cause for alarm. However, certain patterns of decelerations, abrupt changes, or erratic variability during labor is often a sign that something is wrong.
Common issues that can affect the baby’s heart rate include:
- The use of general anesthesia
- Usage of labor-inducing medications
- Problems with the placenta
- Umbilical cord complications, including compression or nuchal cord
- Lack of oxygen
- Abnormal uterine contractions (uterine hyperstimulation or tachysystole)
Regardless of the situation, fetal heart monitoring is an essential tool during childbirth. The results can alert obstetricians, maternal-fetal medicine specialists, nurses, and other healthcare professionals when a baby is in fetal distress.
Some mothers with high-risk pregnancies enter labor with preexisting signs that they might have complications. But even women with low-risk pregnancies need fetal heart rate monitoring during labor. In fact, fetal heart monitoring is the most common obstetric procedure in the United States.
Types of Fetal Monitoring
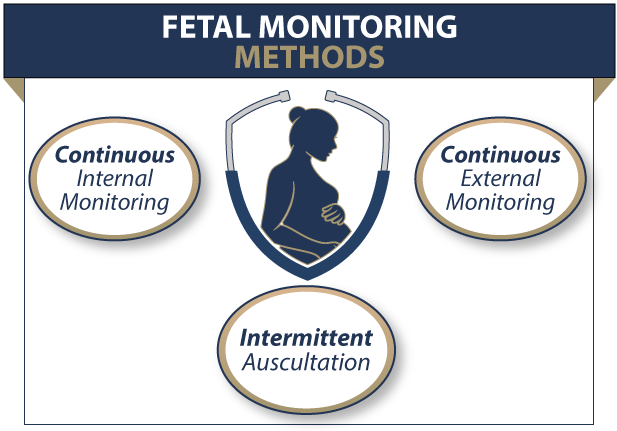
The methods a physician may use to monitor fetal heart rates might differ based on the mother’s known medical conditions:
Electric Doppler Transducer

In the past, medical providers would use only intermittent auscultation to monitor fetal heart rates. “Auscultation” means listening to someone’s body sounds, including their lungs and heartbeat. Doctors, nurses, and midwives typically used special stethoscopes to check the baby’s heartbeat.
Now, the development of modern technology has changed the standard of care. Healthcare providers now use an electronic Doppler transducer attached to the mother’s abdomen to monitor the baby’s heart rate. Sometimes they attach another transducer to the baby’s scalp for closer monitoring. The transducer sends and receives sound waves, then amplifies the sounds created by the baby’s heartbeats.
There are two categories for this type of monitoring:
External Fetal Heart Rate Monitoring

External monitoring involves staff members placing two belts around the mother’s abdomen. Transducers on the belts electronically monitor the fetal heart rate and maternal uterine contractions.
Sometimes medical professionals conduct external monitoring during the third trimester of pregnancy using nonstress tests.
Internal Fetal Heart Rate Monitoring
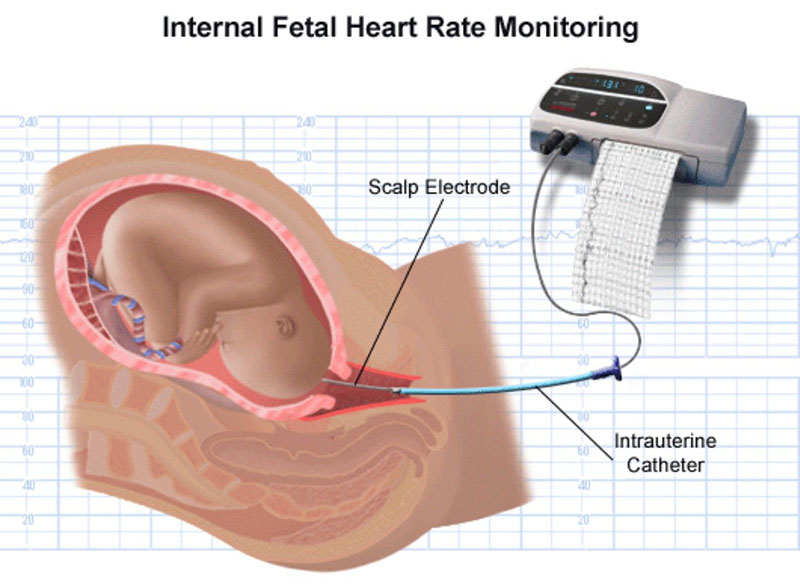
Doctors can only use this method after the mother’s water breaks. The doctor or nurse will insert a wire through the cervix and into the mother’s uterus. They then attach an electrode to the fetus, usually on the scalp. The electrode transmits data helping doctors to monitor the baby more closely.
Doctors may also insert a catheter into the mother’s uterus that checks uterine pressure during contractions. A new, wireless fetal heart monitor is available at some hospitals or for at-home use. As technology develops, these wireless monitors might be useful for telemedicine during online doctor’s appointments and in hospitals during childbirth.
Only trained staff members should use fetal and maternal monitoring equipment. When healthcare providers perform incorrect monitoring or misinterpret the results, it can cause adverse perinatal and neonatal outcomes. The result can be severe brain damage, hypoxic-ischemic encephalopathy (HIE), cerebral palsy, or, in severe cases, death.
How to Interpret Fetal Heart Rate Monitoring
A baby’s fetal heart rate has the following characteristics: the baseline, accelerations, decelerations, and variability.
A baseline fetal heart rate is the baby’s average heart rate over a 10-minute period. This excludes massive jumps or dips in response to contractions. If this baseline is higher than 160 bpm, it is indicative of fetal tachycardia. When the baseline is lower than 110 bpm, it is typically a sign of fetal bradycardia.
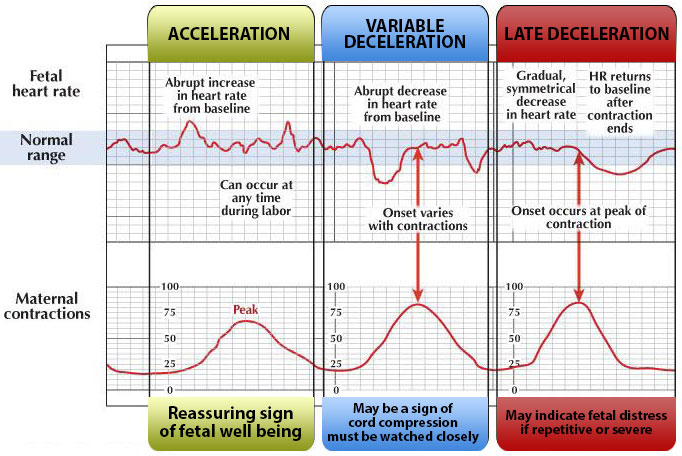
An acceleration is a temporary spike in the baby’s heart rate, typically as a response to fetal movement or a contraction. Accelerations are generally a reassuring sign of the baby’s wellbeing and adequate oxygen supply.
Fetal Heart Rate Decelerations
A deceleration is a temporary drop in the baby’s heart rate. Decelerations can either be reassuring or non-reassuring, depending on when and why they occur:
- Early decelerations are heart rate dips that line up with the mother’s contractions. This is normal and healthy if the heart rate jumps back to the baseline afterward.
- Variable decelerations are a pattern of heart rate dips that happen suddenly and abruptly. The more frequent variable decelerations are, the more concerning it becomes.
- Late decelerations are heart rate dips that don’t line up with contractions. They occur when the lowest point of the heart rate comes after the peak of the mother’s contraction. This is abnormal and can indicate some level of fetal distress.
Fetal Heart Rate Variability
Variability in fetal heart rates refers to the minor differences from the baseline rate over several minutes. A baby’s heart rate might accelerate or decelerate but should return to or near its baseline rate. Variability can have several levels:
Absent Variability

- Absent variability means there is very little to no change at all in the heart rate. This is concerning and indicative of oxygen deprivation.
Minimal Variability

- Minimal variability means there are visible fluctuations, but only of 5 bpm or less. Like absent variability, minimal variability can also be concerning and merit further investigation. Moderate Variability.
Moderate Variability

- Moderate variability means visible fluctuations between 6 and 25 bpm. This is a standard and healthy range of variability and often does not indicate an issue (although other factors may point to one).
Marked Variability

- Marked variability means there are large fluctuations exceeding 25 bpm. While this isn’t always cause for concern, this variability may indicate an issue when it is prolonged over extended periods.
Doctors should be watching for fetal heart rates with:
- Baselines lower than 110 bpm or higher than 160 bpm
- Late decelerations after the mother’s contractions
- Heart rates with absent variability or extremely marked variability
Any of the above signs can indicate oxygen deprivation that puts the baby at risk for brain damage at birth.
Classifying Fetal Heart Rates
Medical professionals must communicate clearly and efficiently about a patient’s status. This is particularly true in the type of emergency situations obstetricians, midwives, and nurses encounter during labor and delivery.

The following method of classifying fetal heart rates should assist them in quickly identifying and addressing problems.
Category 1 Fetal Heart Rates
In Category I, the baby’s baseline heart rate is normal between 110 and 160 beats per minute. Their heart rate will also have good variability and no variable or late decelerations.
This reading usually means the fetus has a normal acid-base status, indicating they are not suffering from oxygen deprivation. Unless there are signs of complications, medical staff usually do not need to intervene.
Category 2 Fetal Heart Rates
In Category II, the fetal monitoring strips show any one of the following:
- moderate variability with recurrent late or variable decelerations
- minimal variability with recurrent variable decelerations
- absent variability without recurrent decelerations
- bradycardia with moderate variability
- prolonged decelerations
- Tachycardia
A Category II Fetal Heart Rate Strip is a worrisome sign that the medical staff must closely evaluate. Category II readings that persist could indicate that the doctor should perform a C-section.
Category 3 Fetal Heart Rates
When the fetal heart rate falls into Category III, the baby needs immediate attention. The fetal heart tracings will show:
- Minimal or absent fetal heart rate variability
- Recurrent late decelerations
- Recurrent variable decelerations
- Bradycardia (slow heartbeat)
- Sinusoidal patterns indicate conditions like intrauterine bleeding, severe fetal anemia, Rh disease, severe oxygen deprivation
Doctors must deliver babies in Category III as quickly as possible using assistive delivery methods. Under almost all circumstances, this means performing an emergency C-section.
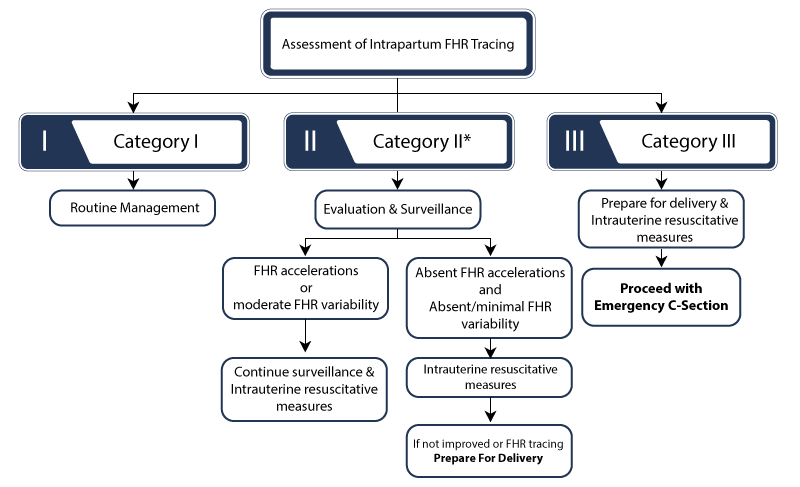
With Category I or Category III readings, the baby’s status is easier to determine. A Category I heart rate probably requires no intervention. On the other hand, Category III requires immediate attention to prevent or minimize the risk of birth injuries.
Category II is more difficult to understand – the baby might or might not be in distress. But a baby’s healthcare providers should show concern when the baby’s heart rate is Category II. Medical professionals must conduct further monitoring and testing to determine if the Category II strip does indicate fetal distress.
Medical staff can try interventions with a Category II baby. However, they must move to delivery when these interventions fail. If they delay action, the baby’s heart rate can escalate into Category III.
If obstetricians and delivery nurses fail to act, the baby can suffer lifelong birth injuries. This includes brain injuries like hypoxic-ischemic encephalopathy, which often lead to a cerebral palsy diagnosis later in childhood.
Where Medical Providers Can Go Wrong

Expecting mothers usually have a team of medical professionals guiding her and her baby through labor and delivery. And childbirth usually occurs in hospitals and other facilities that should have trained staff and adequate equipment.
Even so, the doctors, nurses, midwives, medical staff, and hospitals make mistakes that harm mothers and babies.
Healthcare staff sometimes fail to observe a mother’s progress through labor. It’s especially critical for them to pay attention to the fetal monitoring strips to monitor for fetal distress. When they fail to do so, babies can be susceptible to brain damage, hypoxic-ischemic encephalopathy, and cerebral palsy.
Overlooking troublesome test results and failing to report them to a mother’s physician or midwife can count as medical malpractice.
Hospitals have a responsibility to provide safe, effective care to their patients. But sometimes they fail to train staff properly. Fetal heart monitoring is too important for untrained or under trained personnel to perform.

When hospitals fail to have a properly trained staff, signs of fetal distress on fetal monitoring strips can be missed. In such cases, some state medical malpractice laws allow additional claims against the hospital where the malpractice took place.
Did Medical Malpractice Cause My Child’s Birth Injuries?

Fetal heart rate monitoring is the first line of defense against fetal oxygen deprivation during labor. Proper monitoring can alert medical professionals to a baby in fetal distress before it causes permanent injuries. But failing to monitor, misinterpreting the results, or delayed reactions to non-reassuring results can make these tragic outcomes more likely.
If a family believes medical negligence caused or worsened a child’s injuries, legal support may be an option. A specialized birth injury attorney can review the medical records and circumstances to assess whether a claim exists.
Families who have experienced the effects of brain injuries from missed fetal distress deserve to know whether they were avoidable. Our top rated birth injury lawyers will help you find those answers and obtain the necessary funds to secure treatment.
Our team at Miller Weisbrod Olesky will thoroughly investigate the facts, holding responsible parties accountable by pursuing medical malpractice claims.
What is the Statute of Limitations in a Birth Injury Lawsuit?
A statute of limitations (SOL) is a law that sets a time limit on how long an injured person has to file a lawsuit after an accident. It is essential to understand that statutes of limitations vary based on the case and the state where you file. For instance, the deadline for birth injury claims is typically different from other claims, such as injury to private property.
Generally, the clock starts ticking on the date the injury occurred. However, there are exceptions to this rule. In some cases, the statute of limitations starts when a person discovers or reasonably should have discovered an injury. When dealing with government agencies, SOLs can become even more complex.
For example, if the party that injured you was:
- A federal employee
- Employed by a military hospital, Veterans Administration facility, or a federally funded medical entity
You may need to file a birth injury claim under the Federal Tort Claims Act (FTCA). In FTCA cases, claimants must go through certain administrative procedures before filing a lawsuit. In some states, you may have less time to give notice if:
- The negligent party was a local or state government hospital.
- The doctors and medical providers are employees of a governmental entity.
If you file your case outside of the statute of limitations, the court will typically dismiss it. This means you will not be eligible to recover compensation for you or your child’s injuries.
Determining when a statute of limitations begins on your case can be tricky. If you are considering pursuing compensation for a birth injury, contact an attorney as soon as possible.
How Can Our Birth Injury Attorneys Help?

Doctors can sometimes prevent brain damage at birth by taking quick action in response to non-reassuring fetal heart rates. However, it takes an expert review of the facts of your birth to determine whether medical professionals made preventable errors.
Our Process
Our team of committed birth injury attorneys, nurses and paraprofessionals works to answer these questions and seek compensation. We use our detailed medical negligence case review process to assess your potential birth injury case.
We start by learning more about your pregnancy by gathering records to determine what happened during and after your delivery.
We will call in skilled medical experts who review your records and provide insight into where medical professionals went wrong. If we feel medical negligence caused or worsened your baby’s brain injury, we meet with you to discuss further.
At no point in our legal intake process will we ask you to pay anything. The medical review of your case and the consultation are free. We only receive payment once you do. The sooner you reach out, the sooner we can investigate your case and gather the evidence to support your claim.
We work on a contingency fee basis, meaning you will not pay any legal fees until we win your case. We do not purse any medical malpractice cases unless we fully believe we can win.
Contact us today to schedule your free consultation by calling our toll-free line at (888) 987-0005. You can also reach us by filling out our online request form.
National Birth Injury Law
Our National Birth Injury Attorneys, nurses, and support staff understand that parents of children with birth injuries feel overwhelmed. So, every client has the attention and support of a team of trained, compassionate professionals. But we don’t just offer compassion.
We offer a process to help you discover whether your child’s birth injury, HIE, cerebral palsy or brain injury at birth was caused by medical malpractice.
Call our offices today at (888) 987-0005 for experienced assistance in a free consultation.
Quick Links
Testimonials
- Lyric C. I feel like our voice was heard in a sense of what can possibly go wrong in a delivery and finding us answers. I feel with our settlement, we are now in a comfortable position to provide for our son.
- Lyssa L. They are not just people that say “hey let's get you money and let's go” The law firm was very thorough with us. It was awesome. I don't want to cry, because I think about and it's amazing that they were able to help me and that we were able to help my son and get the story out there.
- Jay C. Throughout the process, one thing was clear to us, the ultimate interest of our child was the utmost concern of Max and his team and as parents navigating a situation like that, that was refreshing to know we had them firmly on our side. I highly recommend them.
Popular Cities
- ★ Dallas Birth Injury
- ★ Houston Birth Injury
- ★ Atlanta Birth Injury
- ★ Chicago Birth Injury
- ★ Philadelphia Birth Injury
Locations
★ Dallas
11551 Forest Central Drive, Ste. 300
Dallas, TX 75243
★ Houston
12929 Gulf Freeway, Ste. 111
Houston, TX 77034