Meconium Aspiration Syndrome
What is Meconium Aspiration Syndrome (MAS)?
Meconium is a baby’s first feces. Meconium aspiration syndrome (MAS) occurs when a mixture of amniotic fluid and meconium gets aspirated into the lungs (i.e., the baby breathes this mixture) around the time of delivery. MAS is a major cause of serious medical complications or death in infants, usually occurring during prolonged or arrested labor or when the baby is born prematurely.
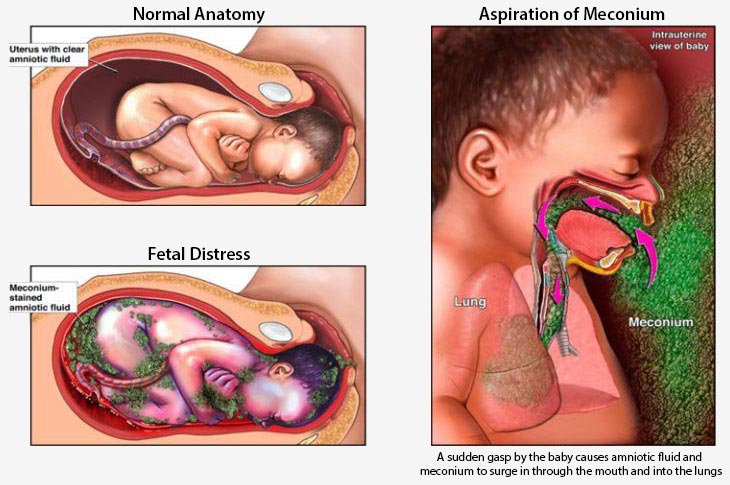
It is notable that meconium lines the intestines of the fetus, even though the fetus does not eat. When oxygen deficiency (hypoxia), infection, or another form of fetal distress causes the baby to gasp for breath, they may inhale meconium mixed with amniotic fluid into their lungs.
Alertness of the medical providers to the signs of MAS can help predict the risk ahead of time and prepare for timely treatment.
When a baby is born with meconium on their face, mouth or inside their throats, doctors and nurses must react quickly to remove the meconium and take other measures including neonatal resuscitation in order to prevent the meconium from being aspirated into their lungs which can cause serious complications. If medical providers fail to take the appropriate steps or fail to use the appropriate equipment, they may be responsible for medical malpractice if a birth injury occurs to the baby.
What is Meconium?
Meconium is a sterile form of fecal stool, dark green in color, which is produced in the intestines prior to birth. In normal conditions, meconium is passed when the newborn begins to feed after birth. But in some cases, the fecal material may be released into the amniotic fluid close to the time of birth.
When the passage of meconium occurs in response to fetal distress, the risk of the baby developing meconium aspiration syndrome is high. In a full-term fetus, the passage of meconium might be normal. But in preterm or post term babies, the meconium noted at the time of delivery is often a sign of abnormality. In some cases, the passage of meconium also occurs if the baby has developed an in-utero infection.

Incidence of MAS
According to studies by National Library of Medicine, the mixing of amniotic fluid with meconium, clinically known as MSAF or meconium staining of the amniotic fluid occurs in about 10 to 15% of the babies. Out of these:
- About 4 to 10% will develop meconium aspiration syndrome
- About one in three babies who develops MAS will need breathing support through ventilator
- About 10% will develop air leak syndrome (air escaping from the lungs to other body parts) due to insufficient ventilation of the immature and fragile lungs
- About 5 to 10% of these neonates will have a fatal outcome
- About 5 to 6% of the babies diagnosed with PPHN (pulmonary hypertension of the newborn that occurs due to restricted lung vessels and oxygen deprivation) may have this condition because of meconium aspiration syndrome
Risks to the Baby’s Health with MAS
Respiratory distress resulting from meconium aspiration syndrome in babies during antepartum (before childbirth) or intrapartum (the period between labor onset and placenta delivery) or the neonatal (just after birth) phases can result in pulmonary effects such as:
- Airway obstruction (air cannot move in and out of the lung airways)
- Chemical pneumonitis (lung inflammation due to inhalation of toxins)
- Pneumonia
- Interference with alvelor gas diffusion (the process of lungs and blood exchanging carbon dioxide and oxygen)
- Surfactant dysfunction (lung disorder resulting from functional or composition abnormalities of the surface-active fats and proteins in the lung tissue)
These pulmonary effects lead to a mismatch of the gross ventilation (air flow) and perfusion (blood flow). This mismatch prevents the optimal oxygen delivery from the lungs to the blood. To further complicate matters, many babies with meconium aspiration syndrome develop PPHN because of the constriction of the lung blood vessels and in-utero stress. Primary or secondary PPHN restricts the amount of oxygen delivered to the brain and other vital organs, increasing the risk of birth asphyxia and cerebral palsy.
Airway obstruction resulting from MAS may cause parts of the baby’s lungs to collapse. This can happen because the air will reach certain areas of the lungs beyond the obstruction, but it will have no way to exit (breathe out). Consequently, over-expansion of the involved lung may occur. As the particular regions of the lung continue to over-expand, it can eventually cause lung rupture. Once this happens, the air will begin to accumulate in the baby’s chest cavity that houses the lung. This life-threatening condition is called pneumothorax, which can lead to complete lung collapse. When this occurs, emergency neonatal resuscitation efforts must be undertaken immediately to avoid a brain injury due to hypoxia or anoxia.
Although the fecal meconium is sterile, it still predisposes the baby to lung infection when it is present in the airways. It is notable that MAS is ultimately a clinical diagnosis. The medical team must always suspect MAS in a baby born in an MSAF environment or born with respiratory distress and prepare for emergency neonatal management.
Causes of Meconium Aspiration Syndrome
When the baby is in the womb, several factors can contribute to increased intestinal activity and sphincter muscle relaxation (which controls bowel movement). This may lead to meconium passage into the amniotic fluid. The resulting mixture is a green-stained, thick fluid. Following this occurrence, if the baby gasps reflexively during labor, delivery or shortly after delivery, they may inhale the meconium mixture into their lungs. This causes the development of meconium aspiration syndrome or MAS.
Risk factors for MAS include:
- Preterm or post term baby
- Fetal distress
- Prolonged or arrested labor
- Infection, such chicken pox or meningitis
- Complications of the umbilical cord
- Baby is small or under-weight for their gestational age
- Poor in-utero development
- Maternal diabetes
- Preeclampsia (maternal hypertension)
- Other chronic medical conditions
- Intra-uterine hypoxia (low levels of oxygen supply to the fetus)
- Maternal substance use
- Failure to remove the meconium and provide neonatal resuscitation
Passage of Meconium due to Fetal Distress
The correlation between meconium stained amniotic fluid (MSAF), fetal distress and hypoxia-anoxia is important to understand. Fetal distress may stimulate the fetus to pass meconium, leading to MSAF. Babies born in the MSAF environment may develop meconium aspiration syndrome. MAS may, in turn, induce hypoxia-anoxia via serious pulmonary effects, such as airway obstruction, chemical pneumonitis, interference with alvelor gas exchange, and surfactant dysfunction.
This is how the MSAF environment is created: Fetal distress during childbirth can trigger colonic activity by enhancing the constriction/relaxation of the intestines (known as intestinal peristalsis) as well as easing of the anal sphincter muscle. This enables the passage of meconium into the amniotic fluid, creating an MSAF milieu.
Preventing Meconium Aspiration Syndrome (MAS)

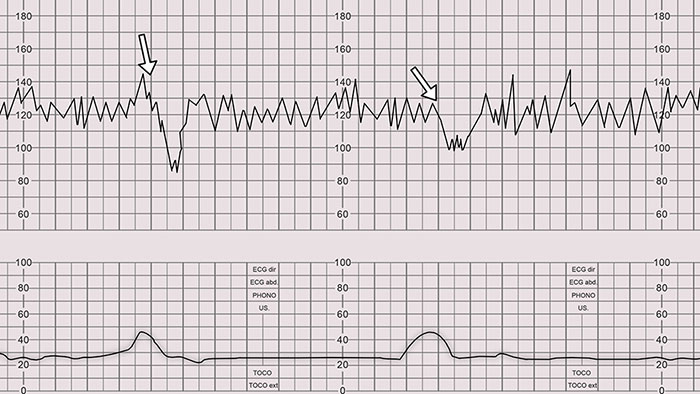
If the medical provider believes that meconium may be present at birth, a care team with specialists should be present at the time of delivery. Signs of meconium may be seen during labor if meconium stained fluid leaks from the birth canal through the vagina or signs of the electronic fetal monitoring strips show that fetal distress—a leading cause of meconium release—is occurring.
When these signs are seen a specialty team of neonatal nurses and doctors should be present in order to quickly prevent or minimize meconium aspiration syndrome (MAS). The number one goal of this specialty team is to prevent any meconium from being pulled into the lungs. If some meconium has already been aspirated before birth, the goal is to stop any additional meconium aspiration and provide neonatal resuscitation efforts immediately.
After childbirth, if the newborn has meconium on their face, mouth or in its throat, the medical team must act fast to remove as much meconium as possible in order to reduce the risk of inhalation or stop additional inhalation of the meconium. The medical provider should immediately suction the nose, mouth and throat. Any delay in suctioning can cause meconium to be sucked in (aspirated) into the lungs so this is an emergency procedure.
If meconium has already been sucked into the throat and the baby is having a difficult time breathing the neonatologists and neonatal nurses may have to insert a laryngoscope (an endoscopic tube) into the baby’s larynx and trachea in an attempt to remove the traces of meconium in those areas with a device called a meconium aspirator. Once the meconium is removed, neonatal resuscitation efforts can help improve the baby’s breathing.

The failure to provide a neonatal team after seeing signs of meconium or the failure of a team to suction and provide neonatal resuscitation in the presence of meconium constitutes medical negligence if a birth injury/brain injury occurs.
Signs & Symptoms of MAS
The signs and symptoms of meconium aspiration syndrome may differ from one baby to another, but some of the common indicators include:
- Labored or rapid breathing
- Breathing in with retraction (pulling in) of the lower chest wall
- Breathing out with grunting sounds
- Cyanosis or bluish color of the skin and lips
- Limp or lethargic body
- Yellowish green color of the umbilical cord, skin or nail beds due to meconium exposure
- Low APGAR score (low rating of the baby’s respiration, reflexes, heart rate, color and muscle tone post-birth)
When these signs and symptoms are apparent at birth, neonatal resuscitation is an emergency requirement to prevent or minimize the damage due to MAS.
Diagnosis of MAS
If the presence of meconium in the amniotic fluid is suspected, the medical providers may try to confirm the diagnosis with:
- Use of stethoscope to detect abnormal breathing sounds in the chest
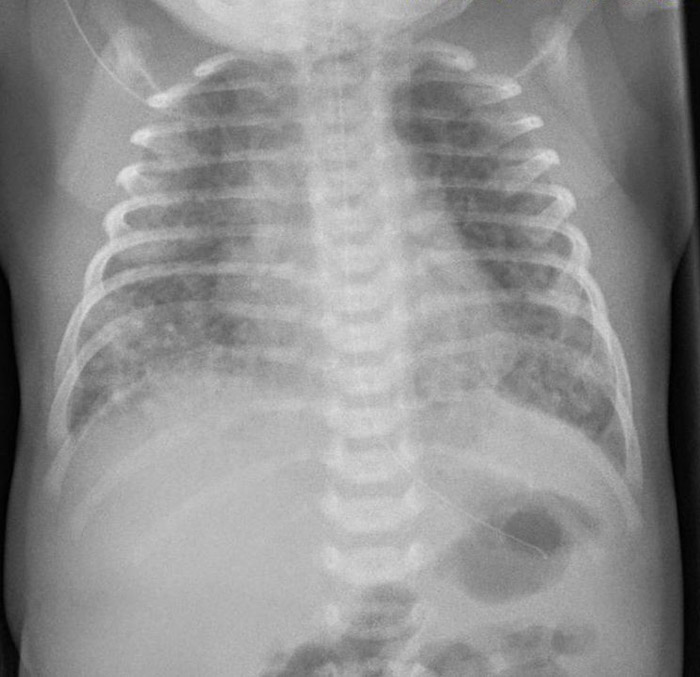
- Chest x-ray to detect respiratory distress (troubled breathing)
- Laryngoscopy to look for traces of meconium staining in the baby’s vocal cords
- Blood culture tests to identify certain types of bacterial infections
Prognosis
Babies diagnosed with severe MAS who require breathing support may experience complications. Infant brain ischemia may occur in some cases, leading to brain damage. Permanent lung damage is rare, but may occur in case of lung rupture or collapse following pulmonary hypertension. In the most severe cases of MAS infant fatality may occur.
Children who have suffered MAS may have a higher risk of developing an asthma-like condition known as “reactive airway disease.” These children may experience shortness of breath, coughing and wheezing, particularly when they are affected by a flu or common cold. The root causes of fetal distress that triggered the meconium passage may impact the prognosis.
Pathophysiology | Functional Disorders Associated with MAS
A number of long-term consequences and disorders are associated with babies that experience MAS. These may include:
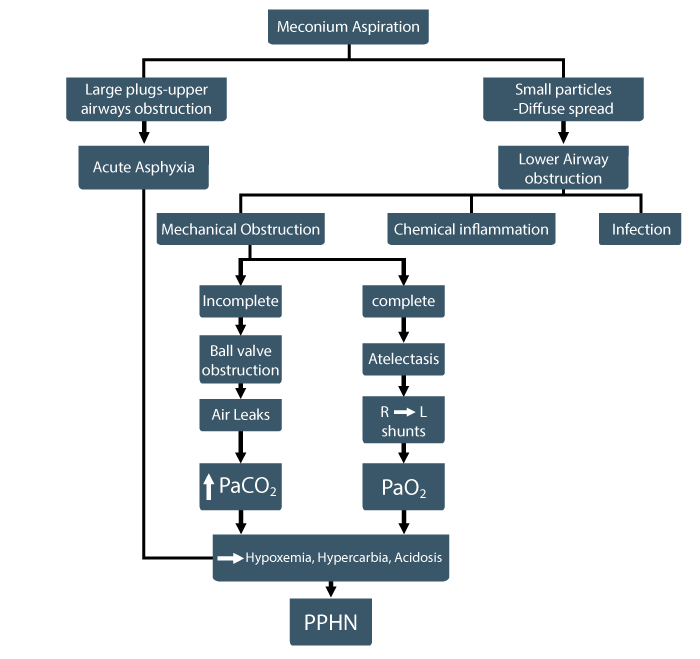
Airway Obstruction
Larger airways experience obstruction within the first 15 minutes of exposure to meconium. This causes reduced lung compliance, increased lung resistance, hypercapnia (carbon dioxide buildup in the blood), acute hypoxemia (low blood oxygen levels), respiratory acidosis (inability of lungs to remove carbon dioxide), and atelectasis (partial lung collapse).
After 60 minutes of meconium aspiration, the obstruction occurs in the smaller airways as the meconium travels to these parts. This triggers pulmonary edema (excess fluid accumulation in the lung tissue), lung inflammation, vasoconstriction (blood vessel constriction in the lungs), bronchoconstriction (narrowing of the airways), and airways collapse.
Fetal Hypoxia
The parts of the baby’s lungs that only partially participate or don’t participate in ventilation due to airway obstruction due to MAA will become hypoxic. This may lead to an inflammatory response. Partial obstruction will cause hyperinflation and air trapping in some parts of the lungs, followed by pneumothorax. In case of chronic hypoxia, circulatory and respiratory failure may occur because of increased PPHN (persistent pulmonary hypertension in the newborn). This hypoxia will begin to result in a brain damage due to the lack of oxygen and can result in the baby suffering from hypoxic ischemic encephalopathy (HIE) which is a leading cause of cerebral palsy.
Infection
Pathogens such as Gram-negative rods (bacteria resistant to multiple drugs) and endotoxins (toxins found in the bacterial walls) are more likely to be present in meconium stained amniotic fluid (MSAF) compared to clear amniotic fluid. Babies born in MSAF environments more commonly experience a microbial invasion of the amniotic activity or MIAC. This may trigger an inflammatory response and intra-amniotic infection, leading to fetal lung inflammation.
Pulmonary Inflammation
Pro-inflammatory cytokines (proteins affecting the inflammatory response) often originate in meconium, which may directly or indirectly lead to lung tissue injury in the baby. For instance, they may be responsible for the release of proteolytic enzymes (enzymes which breakdown proteins). These enzymes may damage the delicate lung membrane. In addition, activated cytokines and leukocytes (white blood cells) may produce reactive oxygen and nitrogen species with cytotoxic effects (toxic to the living cells in the lungs.)
Surfactant Inactivation
Surfactant is a surface-active agent that reduces surface tension to enable lung expansion when the baby breathes in air and prevent atelectasis (full or partial lung collapse) and lung edema. Surfactant also defends the lungs as an anti-inflammatory agent.
Depending on the meconium and surfactant concentration, the surfactant inhibition may be moderate or severe. When the surfactant concentration is relatively low, its inactivation may occur even with significantly diluted meconium. Meconium can prevent the surfactant from spreading over the tiny air sacs in the lungs, triggering lung collapse or lung edema.
Persistent Pulmonary Hypertension in Newborns (PPHN)
After birth, if the blood circulation in newborn fails to adapt to the conditions outside the womb, it may cause PPHN. A significant number of babies with meconium aspiration syndrome will develop PPHN. Depending on the meconium concentration in the respiratory tract, PPHN may develop from a combination of hypoxia, vasoconstriction, and a mismatch of the ventilation-perfusion. PPHN is one of the leading causes of fatal outcomes in babies with MAS.
Treatment of Meconium Aspiration Syndrome
Meconium and its impact on a baby has remained an enigmatic phenomenon for medical researchers ever since the Greek philosopher Aristotle coined the term (“meconium arion” in Greek means “opium like” – a substance that Aristotle believed induced fetal sleep.) Medical advances have improved the medical community’s understanding of optimal predictive measures, neonatal resuscitation techniques, and subsequent management approaches for the severely ill babies with meconium aspiration syndrome.
However, what is quite clear is that early detection can make a key difference. If the baby is experiencing fetal distress, careful fetal monitoring can alert the medical team to the possibility of MAS.
CPAP
Continuous positive airway pressure or CPAP to support breathing may be required in neonates with severe MAS. In this case, a breathing tube will be inserted in the newborn’s windpipe after birth, and they will be placed on a CPAP machine. CPAP helps the baby breathe on their own through prongs placed within the nostrils, while the machine delivers pressurized air, with or without supplemental oxygen.
High Frequency Ventilation
High frequency ventilation or HFV is a relatively new ventilation technique that involves the use of high respiratory rates compared to normal breathing. HFV enables successful gas exchange (air exchange at low volumes) and is known to be a useful MAS treatment. The advantages of HFV include reduced barotraumas (lung injury caused by barometric air pressure fluctuations), faster generation of airway secretions, and fewer changes in the lung tissue.
Surfactant Therapy
This treatment involves the delivery of intermittent, repetitive high doses of surfactant to the baby with MAS. It’s known to improve oxygenation, reduce the air leaks, resolve PPHN, and lower the duration of ventilation. Surfactant therapy is a significant advance in MAS care, and it can reduce mortality and morbidity in severe cases. Moreover, the therapy should be selectively used in MAS, when the treatment is started early in newborns with severe disease.
Inhaled Nitric Oxide
Inhaled nitric oxide (INO) is an important management modality for PPHN, which is often associated with MAS. It can lower the resistance of blood vessels in the lungs and reduce lung edema. Effective INO use in recommended dosage – usually 20 PPM (parts per million) – requires sufficient lung expansion so that the dosage delivery in the lungs can be optimized. Therefore, the use of mechanical ventilation is necessary to achieve the maximum benefits of INO therapy in babies with MAS.
Extra Corporeal Membrane Oxygenation
Extra corporeal membrane oxygenation or ECMO is considered an effective tool to reduce disability and death in babies with MAS. Research shows that the incidence of complications is lower when ECMO is used. The ECMO device involves the use of a pump that functions like an artificial lung. Similar to a biological lung, it adds oxygen to the pumped blood, and takes out carbon dioxide. Thereafter, it delivers the oxygenated blood back to the baby.
Supportive Care
Babies with severe MAS require careful handling because they can be easily agitated and quickly become acidotic (too much acid in the body) and hypoxemic (too little oxygen in the body). An optimum thermal environment should be maintained. The medical team should carefully monitor the baby’s blood volume and systemic (arterial) blood pressure. To ensure that the pulmonary (lung) blood pressure remains lower than the systemic blood pressure, the use of blood transfusion therapy (delivering blood intravenously) and systemic vasopressors (device to restore normal blood pressure) may be necessary.
Is Your Child’s Meconium Aspiration Syndrome the Result of Medical Malpractice?
Parents whose children suffer from meconium aspiration syndrome deserve an answer to how their child developed this condition and whether it was preventable. Our dedicated birth injury lawyers can help you find out if medical providers missed important signs of meconium prior to birth or failed to respond to the presence of meconium at the time of birth.
If your child has been diagnosed with MAS or suffered a birth injury including HIE or cerebral palsy, and you suspect this may have been caused in part by medical mistakes, Miller Weisbrod Olesky will thoroughly investigate the facts and hold responsible medical providers accountable by pursuing medical malpractice claims against them. The compensation our clients receive helps them pay for their child’s current and future medical appointments, physical and occupational therapy, equipment needed to help cope with any disabilities, and the other expenses associated with caring for a child with brain injuries, seizure disorders, organ damage, speech, vision, hearing or motor impairments, and cerebral palsy caused by MAS.
Sometimes families are hesitant to reach out to a medical negligence and birth injury law firm. Other parents feel overwhelmed by their challenges and are concerned that they will not be able to help out in a lawsuit involving their child’s birth injury.
Why Should You Talk with the Knowledgeable Attorneys at Miller Weisbrod Olesky?
The only way to find out if you have a birth injury case is to talk to an attorney who understands birth injuries caused by meconium aspiration syndrome (MAS).
At Miller Weisbrod Olesky, a team of committed attorneys, nurses and paraprofessionals uses our detailed medical negligence case review process to assess your potential claim. We start by learning more about you and your child and the status of meeting/missing developmental milestones. Then we gather medical records to determine what happened before, during, and after your delivery. We call in skilled medical experts who review your records and let us know if they think medical errors could have caused your child’s injuries.
If we feel medical negligence caused or contributed to your child’s injuries, we meet with you to discuss how you can receive compensation from the medical professionals who made the errors.
At no point in our legal intake process will we ask you to pay anything. The medical review of your case and the consultation are free. We only receive payment when you do.
Miller Weisbrod Olesky is different from most law firms.
We provide help NOW.
Many attorneys focus only on pursuing their client’s legal case. At Miller Weisbrod Olesky, we know your child needs help today – not just when your birth injury lawsuit is settled. We have a team focused on helping our clients NOW when they need it most.

We know that children with birth injuries like hypoxic-ischemic encephalopathy (HIE) and cerebral palsy often require intense therapy, specialized medical treatment, and assistive care. The stress of providing for a birth injured child’s needs can be both emotionally and financially draining.
But just ‘knowing’ this is not enough. We act on this knowledge by providing exceptional services to birth-injured children and their families.
While Miller Weisbrod Olesky’s birth injury attorneys aggressively prepare each legal case, another department goes into action to help the families of children we represent. Led by a nurse-attorney, this department acts as a medical case manager for our birth injury clients by:
- Regularly monitoring the child’s medical treatment status,
- Helping facilitate medical treatment and therapy, and
- Arranging transportation and services.
Where necessary, we also help families locate local medical providers specializing in the care and treatment of children who have suffered a birth injury. With Miller Weisbrod Olesky, you’re not just a ‘case’. And that’s important when you’re looking for a lawyer who can help you cope with your child’s needs today.
Please call or email us today to get started.
Registered Nurses and Nurse-Attorneys Are a Vital Part of Our Birth Injury Team … and Yours

Most national birth injury law firms will employ one or two nurses to assist the review of cases and medical research. But Miller Weisbrod Olesky offers an unmatched number of nurses and nurse-attorney employees support to both the birth injury attorneys and our clients.
Our team of registered nursing staff and nurse-attorneys bring a deep level of medical and personal insight to every client’s case. Our nursing team includes both an experienced labor and delivery nurse as well as an ICU nurse. Working closely with the rest of the team, they investigate the reasons behind a birth injury and how medical professionals breached their standard of care.
Why Should You Talk with the Knowledgeable Attorneys at Miller Weisbrod Olesky?

The only way to find out if you have a birth injury case is to talk to a medical negligence attorney who understands how ischemia occurs during labor and delivery, birth and shortly after birth if baby’s are not correctly monitored, diagnosed and treated.
At Miller Weisbrod Olesky, a team of committed attorneys, nurses and paraprofessionals uses our detailed medical negligence case review process to assess your potential claim. We start by learning more about you and your child and the status of meeting/missing developmental milestones. Then we gather medical records to determine what happened before, during, and after your delivery. We call in skilled medical experts who review your records and let us know if they think medical errors could have caused your child’s injuries.
If we feel medical negligence caused or contributed to your child’s injuries, we meet with you to discuss how you can receive compensation from the medical professionals who made the errors.
At no point in our legal intake process will we ask you to pay anything. The medical review of your case and the consultation are free. We only receive payment when you do.
Contact Our National Birth Injury Lawyers
National Birth Injury Law
Our National Birth Injury Attorneys, nurses, and support staff understand that parents of children with birth injuries feel overwhelmed. So, every client has the attention and support of a team of trained, compassionate professionals. But we don’t just offer compassion.
We offer a process to help you discover whether your child’s birth injury, HIE, cerebral palsy or brain injury at birth was caused by medical malpractice.
Call our offices today at (888) 987-0005 for experienced assistance in a free consultation.
Quick Links
Testimonials
- Lyric C. I feel like our voice was heard in a sense of what can possibly go wrong in a delivery and finding us answers. I feel with our settlement, we are now in a comfortable position to provide for our son.
- Lyssa L. They are not just people that say “hey let's get you money and let's go” The law firm was very thorough with us. It was awesome. I don't want to cry, because I think about and it's amazing that they were able to help me and that we were able to help my son and get the story out there.
- Jay C. Throughout the process, one thing was clear to us, the ultimate interest of our child was the utmost concern of Max and his team and as parents navigating a situation like that, that was refreshing to know we had them firmly on our side. I highly recommend them.
Popular Cities
- ★ Dallas Birth Injury
- ★ Houston Birth Injury
- ★ Atlanta Birth Injury
- ★ Chicago Birth Injury
- ★ Philadelphia Birth Injury
Locations
★ Dallas
11551 Forest Central Drive, Ste. 300
Dallas, TX 75243
★ Houston
12929 Gulf Freeway, Ste. 111
Houston, TX 77034