Diagnosing HIE
HIE Diagnosis
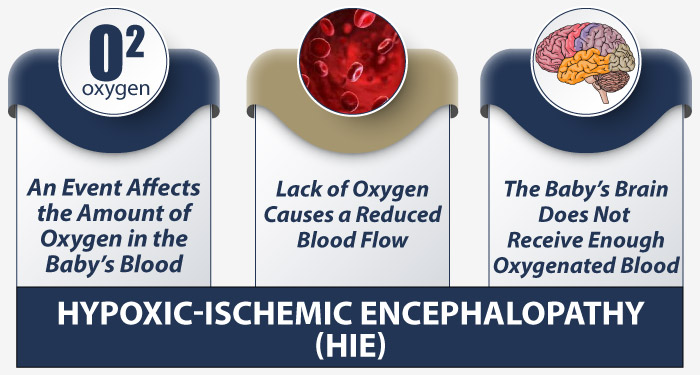
Hypoxic ischemic encephalopathy (HIE) is typically diagnosed within the first few hours of a baby being born. Just like with all brain injuries, early detection and treatment is key to preventing further irreversible harm for the child. But sometimes, medical negligence can delay a baby’s diagnosis and impede critical intervention.
Without a timely diagnosis, HIE can go untreated and progress to more severe stages of brain damage. When doctors miss the signs of HIE or wait too long to start treatment like therapeutic hypothermia, it can constitute medical malpractice.
Over the past three decades, the nationally recognized team of birth injury lawyers, registered nurses, and nurse-attorneys at Miller Weisbrod Olesky have established a proven track record of delivering justice for children and families across the United States who have suffered from all types of birth injuries.
Free Legal Consultation
HIE Injury Lawyers Near You
(888) 987-0005Our Specialized HIE Injury Lawyers are available to meet you in your home or the hospital.
We are prepared to meticulously investigate the circumstances of your case, gather crucial medical records, consult with top medical experts, and fight tirelessly to secure the compensation you deserve for your child's birth injury with no upfront cost to you.
We work on a contingency fee basis, meaning you won't pay any legal fees unless we win your case. We only receive payment once you do.
How is HIE Diagnosed?
A combination of different tests, scans, and observation-based evidence can contribute to an HIE diagnosis after birth.

HIE is typically diagnosed within the first six hours after the baby is born. Sometimes doctors may order additional testing to confirm a suspected case, delaying the official diagnosis by a few days or even up to a week. Before that, though, doctors should inform the mother of their initial concerns and move forward with admission to the neonatal intensive care unit (NICU).
Some diagnostic tests (such as blood testing and spinal fluid testing) may take several days for results, and other testing (such as MRIs and other neuroimaging) may not be safe to conduct until the newborn is at least a few days old.
But doctors should already have a clear idea of whether a newborn is at risk for brain damage at birth based off of the details of the mother’s labor and delivery. All other testing will be used to support those suspicions of an HIE injury and confirm a diagnosis.
Diagnosing HIE from Physical Examination
Babies will typically display symptoms of HIE immediately upon birth. Some of these symptoms include low muscle tone (appearing “floppy”), shallow breathing, a weak cry, and limited to no response to their external surroundings. However, there will often be signs before birth that brain damage has occurred.
OB-GYNs, nurses, midwives, and all other medical professionals must carefully monitor the mother’s pregnancy and labor for signs of HIE that appear before birth.
Examining Pregnancy and Labor
Examining a mother’s physical conditions during pregnancy and labor is the first step in assessing her child’s birth injury risk factors.
Proper prenatal testing should be conducted early on to check the mother for any pregnancy complications that may qualify her pregnancy as “high risk”.
Examples of these types of complications include problems with the umbilical cord, fetal size abnormalities like macrosomia, or the baby resting in an abnormal fetal position in the third trimester.

When these types of pregnancy complications are caught early, it gives healthcare providers time to plan for how to best prepare for the baby’s delivery. This may include administering labor-inducing medications or planning a C-section delivery in advance.
A mother’s labor and delivery is perhaps even more important to monitor for HIE risk factors as it is the time when babies are most vulnerable to suffering from oxygen deprivation and birth asphyxia.
During labor, the uterus contracts to slowly push the baby out through the mother’s birth canal and into the world. During this process, the contractions temporarily restrict the flow of oxygen through the umbilical cord. This happens in all pregnancies, but it can become dangerous for the baby when labor becomes prolonged or arrested.

Prolonged or arrested labor can stem from a variety of causes, including macrosomia, cephalopelvic disproportion, uterine hyperstimulation, or abnormal fetal positioning like breech position.
When this happens, fetal heart rate monitoring is a key indicator of how these labor and delivery complications are affecting the baby’s oxygen supply. Concerning heart rate patterns like late decelerations or absent variability can indicate that the baby is in fetal distress and not receiving adequate oxygen nor blood flow.
Witnessing non-reassuring fetal heart rates can often be the first in a series of signs that will point to a child’s potential HIE diagnosis. To minimize the impact these complications will have on the baby’s brain function, healthcare providers must closely observe the mother’s labor as it progresses and intervene when necessary by inducing labor, assisting labor by using delivery instruments, or ordering an emergency C-section delivery.
APGAR Scores
An APGAR score is a routine assessment tool used for all deliveries to assess a baby’s status at birth and to determine whether or not they will need additional care. It consists of 5 categories:
- Appearance: Does the baby have an abnormal bluish-gray tint to their skin?
- Pulse: Is the baby’s heart rate above or below 100 beats per minute?
- Grimace: Is the baby showing any reflex or reaction to external stimuli?
- Activity: Is the baby showing signs of adequate muscle tone?
- Respiration: Does the baby have a weak cry or a slow and irregular breathing pattern?
A score from zero to two is assigned for each category. Doctors should typically assign the initial score one minute after birth, and then again at 5 minutes after birth.
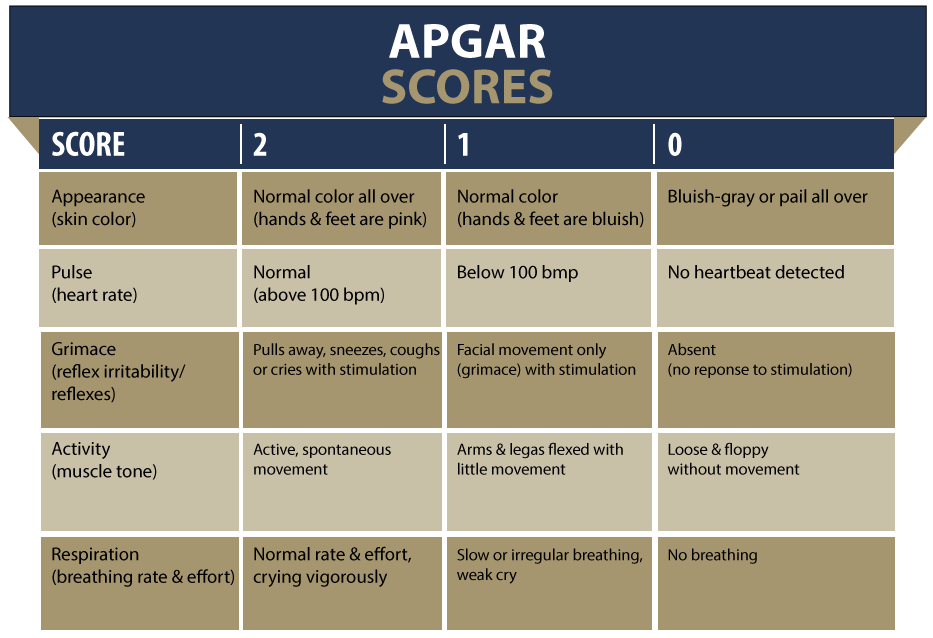
APGAR scores in the range of 7-10 are considered reassuring. Anything below a 7 should be cause for concern and indicate that additional care will be needed. If the score falls below a 7 the second time, it may be taken again at 10 minutes.
Babies with HIE who have suffered from birth asphyxia often (but not always) score lower in all categories of the APGAR score, commonly displaying the following symptoms:
- Their lips may appear blue around the edges
- They may appear overly fussy or cry more frequently than a normal newborn
- They may display signs of apnea (momentary lapses in breathing)
- They may show lower reflexes in response to stimuli
While not a definitive diagnostic tool on its own, the APGAR score is a way to translate physical observations into a quantitative benchmark for birth injuries like respiratory distress syndrome and HIE.
It should be remembered that APGAR scores are determined by the subjective observations of medical providers, so there may be errors made that artificially inflate APGAR scores. It is seen time and time again that APGAR scores that do not match up with the parents’ observations at birth or even photographs and video recordings of the baby at birth.
When medical professionals assign inflated APGAR scores to a baby showing critical signs of needing additional care, it can delay an HIE diagnosis and constitute medical malpractice.
Further Analysis & Antenatal Checkups
Further signs of hypoxic ischemic encephalopathy can come with time as the child ages. Scheduled antenatal checkups are routine so healthcare providers can monitor the baby and check for any physical or behavioral anomalies.
One of the most common indicators of HIE in children is missed developmental milestones.

It’s true that children sometimes progress at slightly different rates. One nine-month-old might be walking while another is just starting to crawl. However, a baby or child who misses several milestones is cause for concern.
By two months, most babies will begin holding their head up and moving their arms and legs more smoothly. They may begin showing reactions by looking in the direction of sounds and following objects with their eyes. These milestones are likely to be absent in a child with an HIE injury.
Later on, children with HIE may show other significant developmental delays such as stunted growth, poor coordination, vision impairments, or impairments to motor and cognitive functioning.
While a child is likely to be given an HIE diagnosis long before these impairments, developmental delays can reveal the severity of their brain injury and the likelihood of concurrent disabilities such as cerebral palsy.
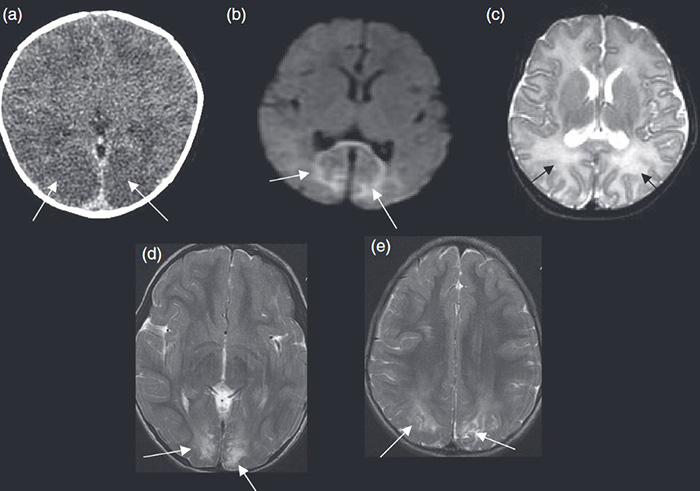
Diagnosing HIE Using Brain Imaging
Advancements in medical technology have allowed medical professionals a new way to catch and diagnose HIE: neuroimaging tests. Neuroimaging allows doctors to see a detailed reconstruction of a patient’s brain anatomy to assess any potential damage to the structures of the central nervous system.
There are a couple different brain injury patterns associated with HIE; the type of pattern will depend on the specific kind of birth asphyxia that caused the injury.
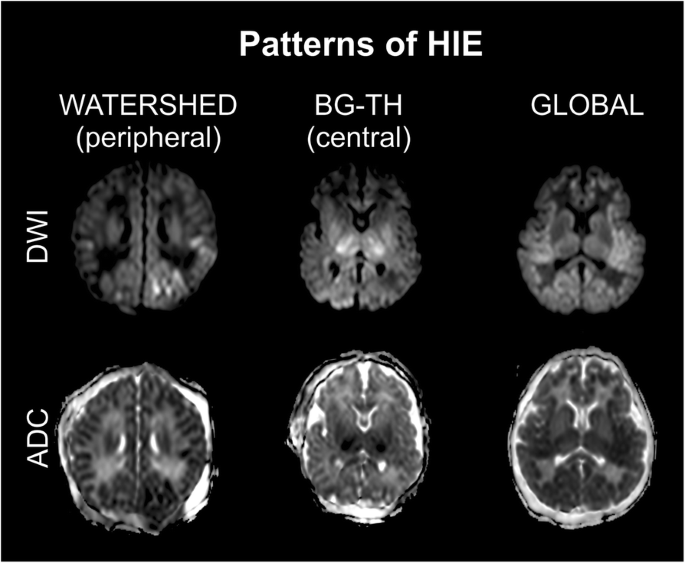
The most common brain injury pattern affects the basal ganglia and thalamus (BG-TH brain injury pattern), the two parts of the brain with the highest demand for oxygen to operate. When a birth asphyxia injury is partial prolonged, meaning the oxygen cutoff was gradual and continued over a certain period, such as with injuries like umbilical cord compression, the blood flow will be able to reach some parts of the brain and not others.
This can result in what’s known as a white matter watershed (WM/WS or parasagittal) brain injury pattern, which indicates damage along the brain’s vascular border zones.
When a birth asphyxia injury is considered acute abrupt, meaning the oxygen cutoff is total and happened suddenly from one specific event (such as a placental abruption), it can create a near total brain injury pattern (also known as a global brain injury pattern). When the entire brain is affected like this, the newborn is at a high risk for death and may not be well enough to get scanned right away.
Neuroimaging tools can take scans of the newborn’s brain for doctors to analyze and determine if they line up with any of these common HIE injury patterns. Listed below are the most common tools doctors may use to diagnose an HIE injury:
Magnetic Resonance Imaging Scan
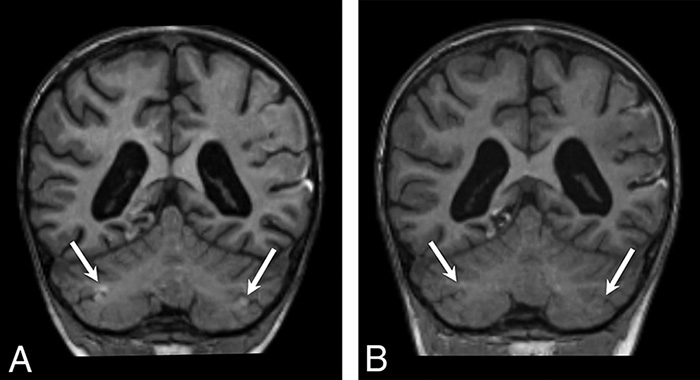
Dubbed as “the gold standard” for assessing brain injuries in infants with HIE, magnetic resonance imaging (MRI) scans are a painless and non-invasive technique for producing detailed 3-D anatomical images of the brain and body.

Rather than using radiation like X-rays and CT scans, MRI scans use metal rods and electric currents to create a temporary magnetic field within the baby’s body.
A transmitter sends radio waves through the body, causing small disruptions and shifts of hydrogen atoms in the brain. These small shifts of atoms emit their own radio waves as they return to their original placement.
Then, a receiver within the MRI machine detects these waves and translates the signals into detailed images. Hundreds to thousands of images are taken and then layered to create a three-dimensional visualization.
HIE injuries will present on the scan as brighter, reflecting higher intensity of the electrical signals in that area of the brain. Conversely, lower intensity in the white matter brain tissue can also identify an HIE injury.
Because there is minimal risk and no exposure to radiation, infants can undergo an MRI screening very soon after birth, usually within the first week.
Doctors must be familiar with MRI scan results and know what to look for when analyzing brain imaging for newborns. Incorrectly interpreting the results can lead to a delayed diagnosis and be grounds for a medical malpractice claim.
Electroencephalography (EEG) Test
An electroencephalography (or EEG) test was the first non-invasive neuroimaging technique developed to measure brain activity levels and diagnose a number of conditions, including neonatal seizures (epilepsy) and traumatic brain injuries like HIE.
An EEG works by placing small metal disks with thin wires called electrodes onto the baby’s scalp with special glue and/or within a special cap. The electrodes detect and record electrical signals produced by the brain, which come through as a series of brain waves for doctors to interpret.

The test is painless and generally very safe, with a low risk of possible complications. During the procedure, no amount of electrical current will enter the baby’s body.
Studies have supported that early EEG scans are a reliable predictor of outcome in HIE. However, compared to older children and adults, the interpretation of the electrical brain waves in a newborn is more complex due to the immaturity of their developing brain. An EEG can help pediatric neurology clinicians identify seizures or understand the impact of injuries to the infant's brain.
Cranial Ultrasound
A cranial ultrasound is a non-invasive medical test that uses reflected sound waves to make pictures of its inner fluid chambers (ventricles) and the cerebrospinal fluid that flows through these chambers. Sound waves and a small probe (called a transducer) produce a picture of the inside of the baby’s body.
Just like an ultrasound of the mother’s womb during prenatal testing, the technologist applies a small amount of gel to the area under examination and presses the transducer against the area under examination.

Cranial head ultrasounds are one of the preferred neuroimaging methods for examining newborn brains because their skull bones have not yet fused together and can sometimes block the passage of ultrasound waves.
Along with being used to detect hypoxic-ischemic events, they can also identify other neonatal head injuries such as hydrocephalus and intracranial hemorrhages (brain bleeds).
Diagnosing HIE Using Blood Testing
Newborn blood tests can reveal vital information about their wellbeing. Oxygen travels through the blood, so babies suspected of having HIE will need their blood drawn for doctors to analyze its contents and identify abnormally low levels of oxygen.
Along with other general tests like hearing and heart screenings, blood samples should be taken within one to two days of the baby’s birth so that results can come back as quickly as possible.
Umbilical Cord Blood Gas Testing
During pregnancy, the baby receives all blood, oxygen, and nutrients from the mother through the umbilical cord. When doctors suspect that a baby may have undergone a hypoxic event during pregnancy or during labor and delivery, they may decide to test the umbilical cord blood gas to gather more information.
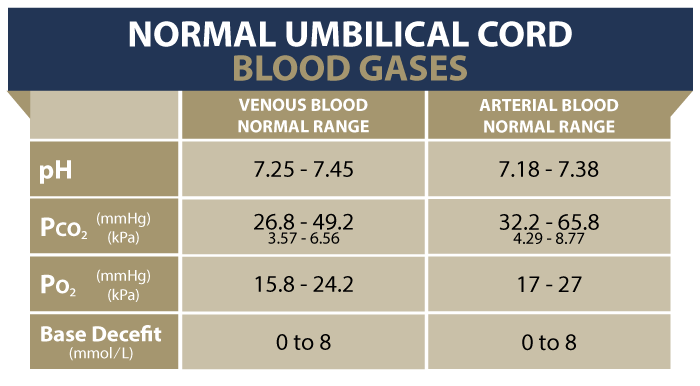
Cord blood gas test results are valuable in birth injury cases because they provide measurable objective evidence of birth asphyxia. When the baby’s tissue cells are significantly depleted of oxygen, the accumulation of metabolic acids in the bloodstream (primarily lactic acid) causes the pH levels to fall.
Cord blood can be tested for pH balance, and if it leans acidic (low or below a pH of 7) it can be a sign that the baby is experiencing fetal acidosis.
Research studies have shown that umbilical cord blood analysis in conjunction with other measurements, such as non-reassuring fetal heart rate readings, low APGAR scores and MRI neuroimaging can be used to determine if the baby has suffered from hypoxic-ischemic encephalopathy. This information is critical to determine when medical treatment (such as therapeutic hypothermia cooling) needs to be started to prevent or lessen brain damage at birth.
About Umbilical Cord Gas Testing
Blood Cultures & Complete Blood Counts
It is common practice for doctors to take general blood culture samples from newborns. When they suspect a case of HIE, taking blood cultures can rule out infections and other birth complications that may be causing symptoms similar to those of a brain injury.

Sometimes, certain neonatal infections can be associated with HIE. These include chorioamnionitis and group B streptococcus, which are both linked to potential brain damage.
According to researchers, perinatal anemia can be one of the underlying causes of moderate or severe birth asphyxia. This may lead to fetal distress during labor and delivery, which is a leading cause of hypoxic-ischemic encephalopathy.
Once born, doctors may conduct a complete blood count (CBC) test to examine the levels of red and white blood cells, hemoglobin, hematocrit, and platelets in an infant’s blood.
They may also decide to test the baby’s cerebrospinal fluid by performing what’s known as a lumbar puncture. Like blood cultures, these kinds of tests can rule out infections and reveal certain biomarkers of brain damage such as observing the presence of proteins in the spinal fluid that are released from damaged neuron cells.
Overall, blood cultures, spinal fluid testing, and complete blood count tests aren’t the primary method for diagnosing HIE, but can be valuable tools to rule out other birth complications and support the initial physical symptoms observed during labor and delivery.
Was My Child’s HIE Diagnosis Delayed or Missed?
Diagnosing hypoxic ischemic encephalopathy in a timely manner is important so that children can begin treatment as soon as possible. When medical negligence delays this diagnosis, it can progress to a more severe stage of HIE and cause further irreversible harm to the child.

If a family believes that any medical mistakes contributed to their child’s delayed diagnosis, legal support may be an option. A specialized birth injury attorney can review the medical records and circumstances to assess whether a viable claim for medical malpractice exists.
Parents whose children suffer from the long-term effects of birth complications, especially HIE and the life changes that come with it, deserve to know whether it could have been prevented or minimized. Our dedicated birth injury lawyers want to help you find those answers and obtain the funds necessary to improve the quality of life for your child.
Sometimes families are hesitant to reach out to a medical malpractice attorney or law firm. They may feel overwhelmed by their circumstances or are worried that a law firm will not be able to help them. But the only way to find out if you have a case is to talk to an attorney who understands how birth injuries can lead to developmental delays and other birth complications that require long-lasting medical support.
What is the Statute of Limitations in a Birth Injury Case?
A statute of limitations (SOL) is a law that sets a time limit on how long an injured person has to file a lawsuit after an accident. It is essential to understand that statutes of limitations vary based on the type of case and the state where it is filed. For instance, the deadline for birth injury claims is typically different from other claims, such as injury to personal property, fraud, contract disputes, and collection of debts.
Generally, the clock starts ticking on the date the injury occurred. However, there are exceptions to this rule, and in some cases, the statute of limitations starts when a person discovers or reasonably should have discovered an injury. When dealing with government agencies, SOLs can become even more complex.
For example, if the party that injured you was:
- A federal employee
- Employed by a military hospital, Veterans Administration facility, or a federally funded medical entity
You may need to file a birth injury claim under the Federal Tort Claims Act (FTCA). In FTCA cases, claimants must go through certain administrative procedures before filing a lawsuit. In some states, if the negligent party was a local or state government hospital or the doctors and medical providers are employees of a governmental entity, the time period in which you must give "notice" may be shorter.
If your case is filed outside of the statute of limitations, it will typically be dismissed, and you will not be eligible to recover compensation for your injuries. Determining when a statute of limitations begins on your case can be tricky. If you're considering pursuing compensation for a birth injury, contacting an attorney as soon as possible is in your best interest.
The Birth Injury Attorneys at Miller Weisbrod Olesky Can Help

It takes a detailed expert review of the facts and circumstances of your pregnancy and your child's birth before determining whether their hypoxic ischemic encephalopathy diagnosis came as the result of medical malpractice.
Our Process
At Miller Weisbrod Olesky, a team of committed birth injury attorneys, nurses and paraprofessionals uses our detailed medical negligence case review process to assess your potential birth injury case.
We start by learning more about you and your child and the status of meeting/missing developmental milestones. Then we gather medical records to determine what happened before, during, and after your delivery. We call in skilled medical experts who review your records and let us know if they think medical errors could have caused your child's injuries.
If we feel medical negligence caused or contributed to your child’s HIE, we meet with you to discuss how you can receive compensation from the medical professionals who made the errors.
At no point in our legal intake process will we ask you to pay anything. The medical review of your case and the consultation are free. We only receive payment when you do. The sooner you reach out to us, the sooner we can begin investigating your case and gathering the evidence needed to support your claim.
We work on a contingency fee basis, meaning you won't pay any legal fees unless we win your case. Contact us today to schedule your free legal consultation by calling our toll-free line at (888) 987-0005 or by filling out our online request form.
National Birth Injury Law
Our National Birth Injury Attorneys, nurses, and support staff understand that parents of children with birth injuries feel overwhelmed. So, every client has the attention and support of a team of trained, compassionate professionals. But we don’t just offer compassion.
We offer a process to help you discover whether your child’s birth injury, HIE, cerebral palsy or brain injury at birth was caused by medical malpractice.
Call our offices today at (888) 987-0005 for experienced assistance in a free consultation.
Quick Links
Testimonials
- Lyric C. I feel like our voice was heard in a sense of what can possibly go wrong in a delivery and finding us answers. I feel with our settlement, we are now in a comfortable position to provide for our son.
- Lyssa L. They are not just people that say “hey let's get you money and let's go” The law firm was very thorough with us. It was awesome. I don't want to cry, because I think about and it's amazing that they were able to help me and that we were able to help my son and get the story out there.
- Jay C. Throughout the process, one thing was clear to us, the ultimate interest of our child was the utmost concern of Max and his team and as parents navigating a situation like that, that was refreshing to know we had them firmly on our side. I highly recommend them.
Popular Cities
- ★ Dallas Birth Injury
- ★ Houston Birth Injury
- ★ Atlanta Birth Injury
- ★ Chicago Birth Injury
- ★ Philadelphia Birth Injury
Locations
★ Dallas
11551 Forest Central Drive, Ste. 300
Dallas, TX 75243
★ Houston
12929 Gulf Freeway, Ste. 111
Houston, TX 77034