Over Ventalation Brain Injury
Over-ventilation in Newborns And Brain Injury
Assisted mechanical ventilation during neonatal resuscitation is a potentially life-saving procedure. The goal is to provide the breathing support to the baby’s lungs, so that oxygen moves from the lungs to the bloodstream, and carbon dioxide passes from the bloodstream to the lungs and out of the baby’s body.

Advanced neonatal ventilator devices allow the neonatal medical providers to precisely measure and deliver controlled amounts of oxygen for babies with respiratory distress. The newborn ventilator devices are complex and should be carefully setup, operated and monitored to ensure safe outcomes.
Improper use or monitoring of neonatal ventilators can cause over-ventilation, which can lead to hypocarbia (excessive removal of carbon dioxide from the bloodstream). When hypocarbia occurs, blood flow in the brain drops quickly which can result in severe damage to the baby’s brain and lungs, including hypoxic-ischemic encephalopathy (HIE) which is the leading cause of cerebral palsy.
Newborn Ventilation Mode and Intensity Factors

Premature babies are already at an increased risk of lung and brain damage because their lungs and other organs are less developed and more delicate. In this condition, the baby cannot sustain over-ventilation, and may suffer from lung injury, brain injury and cerebral inflammation (which can eventually lead to cerebral palsy or mortality.) The higher the intensity of ventilation, the greater will be the baby’s risk of injury.
Medical providers can minimize the risk of ventilation-induced birth injuries if they accurately diagnose the baby’s condition and understand the underlying causes that led to respiratory failure. The medical team that sets-up, operates and monitors the neonatal ventilator device should correctly determine the mode and intensity of newborn ventilation while taking into account the following factors:
- Pulmonary mechanics of the baby (mechanical properties of the newborn’s lung system, including lung volumes, airway pressures, and airflow rate)
- Elastic and resistive forces in the chest wall (the forces that allow the baby’s lungs to expand and contract while breathing)
- Impact of these factors on the inspiratory and expiratory time constant (time taken by the baby to fill the lungs during inhalation and empty the lungs during exhalation)
- Mechanisms of gas exchange in the baby’s lungs (movement of air and blood supply in the lungs)
- Any other primary or secondary birth complications, which may have been identified
An evaluation of these physiological factors allows the medical team to choose the correct mode of mechanical ventilation and the proper ventilation settings to ensure adequate gas exchange and minimize the risk of lung and brain injury.
In particular, premature babies are already at an increased risk of birth injury, simply due to immaturity – which underscores the importance of safe mechanical ventilation to protect the baby.
Interpretation of Ventilator Readings
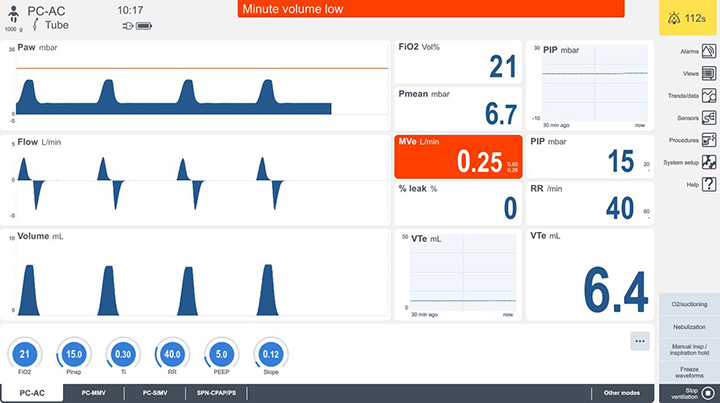
The latest neonatal mechanical ventilators have screen displays to inform the medical providers the precise volume of air that is being delivered into the newborn’s lungs. The ventilator also includes a pressure gauge that enables the medical team to constantly monitor the level of air pressure in the baby’s lungs. The medical team must ensure that two things do not occur (a) too much oxygen is not given to the baby; and (b) oxygen is not delivered too fast to the baby.
But monitoring capabilities of ventilators will only work when the medical team knows how to interpret the readings, correlate them with the baby’s clinical data and signs, is attentive to the changes in data, and makes informed decisions once the data is received.
Any misinterpretation by the medical staff can result in excessive oxygen levels or an excessive rate of oxygen. When either of these occur a significant drop in carbon dioxide levels in the baby’s blood can occur which is known as Hypocarbia.
Hypocarbia, also known as hypocapnia, is a decrease in alveolar and blood carbon dioxide (CO2) levels below the normal reference range of 35 mmHg. CO2 is a metabolic product of the many cellular processes within the body involved in the processing of lipids, carbohydrates, and proteins.
Brain Injuries caused by Over-ventilation and Hypocarbia
Hypocarbia can cause significant brain injury by causing two different injury producing conditions:
- (a) Hemodynamic instability (inadequate blood flow to the baby’s organs, including brain)
- (b) Complex inflammatory cascade (the body’s chemical response to tissue injury) – both of which have a double jeopardy impact on the baby’s brain.
The lack of blood flow due to hypocarbia has also been associated with periventricular leukomalacia (PVL) which involves brain cell death that creates small “holes” in the brain after the cellular death.
Signs of Brain Injury in Newborns from Over-ventilation
Over-ventilation injury to the newborn’s brain may occur during an emergency ventilation procedure in the delivery room (bag ventilation) or in the NICU with a mechanical ventilator. Potential signs that the baby has suffered hypoxic-ischemic encephalopathy (HIE) injury to the brain, cerebral inflammation, or another type of brain damage (which could lead to cerebral palsy) may include:
- Bluish skin tone
- Abnormally low heart rate
- Poor muscle tone and weak reflexes
- Neonatal seizures or other neurologic problems
- Multi-organ malfunction
To confirm the brain injury diagnosis and initiate hypothermia (brain cooling treatment), the medical providers may perform one or more of the following tests:
- Magnetic resonance imaging (MRI)
- Computed tomography (CT) scan
- Electrocardiogram (EKG)
- Electroencephalogram (EEG)
- Echocardiogram
- Cranial ultrasound
- Blood glucose levels
Risks of Over-ventilation Injury in the NICU and Delivery Room

In case of extremely premature babies (born before 28 weeks of gestation), some form of assisted mechanical ventilation is usually required for at least four hours after birth. In many of these cases, the respiratory assistance with ventilation may have to be administered as early as in the delivery room. Considering the elevated risks of brain injury in extremely premature babies, optimal initiation of respiratory support around the time of birth becomes even more critical.
Mechanical ventilation in the delivery room has an increased risk of medical error because protocols and guidelines related to neonatal ventilation may not be properly followed. Moreover, the sophisticated devices available in the neonatal intensive care unit (NICU) may not be available in the delivery room.
Studies have also shown that extended periods of mechanical ventilation in the NICU increase the risks of periventricular leukomalacia (PVL or white matter injury), attention deficit hyperactivity disorder (ADHD), and cerebral palsy in premature babies. Various studies have established that duration of ventilation is a key determinant of neurodevelopmental disorders in babies, including cerebral palsy.
Excessive use of ventilation pressure in the NICU can also cause collapse or scarring of the baby’s lungs, or lead to conditions, such as bronchopulmonary dysplasia or BPD (damage to the airways and air sacs of the lungs) and pneumothorax (full or partial lung collapse). Meconium aspiration syndrome (baby’s inhalation of fecal material) is another potential over-ventilation birth injury.
Is Your Child’s Birth Injury the Result of Medical Malpractice?
Parents whose children suffer from over-ventilation related birth injuries or birth complications want and deserve answers as to cause of their child’s injury and whether mistakes by the doctors and nurses contributed to the injury.
- Were there signs of birth injuries or birth complications during the pregnancy, labor, and delivery process, or presence of risk factors, which were either not recognized or properly treated?
- During the labor and delivery, were there clear indications that their baby was suffering from fetal distress, but appropriate actions were not taken by the obstetrician or nurses?
- Did the neonatal resuscitation team fail to monitor the ventilator and cause overventilation?
- Was excessive, prolonged, or erroneous mechanical ventilation used in the NICU?
- Once there were signs of dropping carbon dioxide levels did the medical providers fail to act appropriately?
- Should brain cooling (also called “hypothermia therapy”) have been offered to your baby, but the doctors and nurses failed to perform the appropriate tests or ignored the results of the tests?
The national birth injury attorneys have extensive experience in all areas of birth injury medical malpractice. The lawyers and nurses at Miller Weisbrod Olesky will help you determine if mistakes of the medical providers caused a birth injury to your child, including Hypoxic-Ischemic Encephalopathy (HIE) or cerebral palsy.
Our award-winning birth injury attorneys have represented families all over the United States in their time of need after a birth injury. We use our experience and expertise to obtain you and your child a medical malpractice settlement that will help provide specialized medical therapy in order to maximize the quality of life and independence of your child throughout their life.
Sometimes families are reluctant to contact a medical malpractice lawyer. It’s also not uncommon for parents to feel overwhelmed by the responsibilities they encounter in caring for their injured child and worried that they will not be able to help out in a lawsuit involving their child’s birth injury. Our birth injury attorneys and nursing staff will address these hesitations and concerns, so you can focus on your child and maximizing their care.
Registered Nurses and Nurse-Attorneys Are a Vital Part of Our Birth Injury Team…and Yours

Most birth injury law firms will employ one or two nurses to assist the review of cases and medical research. But Miller Weisbrod Olesky offers an unmatched number of nurses and nurse-attorney employees support to both the birth injury attorneys and our clients.
Our team of registered nursing staff and nurse-attorneys bring a deep level of medical and personal insight to every client’s case. Our nursing team includes both an experienced labor and delivery nurse as well as an ICU nurse. Working closely with the rest of the team, they investigate the reasons behind a birth injury and how medical professionals breached their standard of care.
Why Should You Talk with the Knowledgeable Attorneys at Miller Weisbrod Olesky?

The only way to find out if you have a birth injury case is to talk to a lawyer experienced in birth injury lawsuits. It’s not uncommon that a birth related complication results in a preventable birth injury, including cerebral palsy, but it takes a detailed expert review by a birth injury attorney of the medical records from your child’s birth to determine if the birth injury was the result of medical malpractice.
At Miller Weisbrod Olesky, a team of committed lawyers, nurses and paralegals uses our detailed medical negligence case review process to assess your child’s potential birth injury case. We start by learning more about you and your child and the status of meeting/missing developmental milestones. Then we gather medical records to determine what happened before, during, and after your delivery. We call in skilled medical experts who review your records and let us know if they think medical errors could have caused your child’s injuries.
If we feel medical negligence caused or contributed to your child’s injuries, we meet with you to discuss how you can receive compensation from the medical professionals who made the errors. Our birth injury attorneys have recovered millions of dollars in settlements for families of children that have suffered a birth injury.
At no point in our legal intake process will we ask you to pay anything. The medical review of your case and the consultation are free. We only receive payment when you do.
Contact Our Birth Injury Lawyers
Miller Weisbrod Olesky
At Miller Weisbrod Olesky, the attorneys, nurses, and staff understand that parents of children with birth injuries feel overwhelmed. So, every client has the attention and support of a team of trained, compassionate professionals. But we don’t just offer compassion.
We offer a process to help you discover whether your child’s birth injury, HIE, cerebral palsy or brain injury was caused by a medical error.
Call our offices today at 888.987.0005 for experienced assistance in a free consultation.
Quick Links
Testimonials
- Lyric C. I feel like our voice was heard in a sense of what can possibly go wrong in a delivery and finding us answers. I feel with our settlement, we are now in a comfortable position to provide for our son.
- Lyssa L. They are not just people that say “hey let's get you money and let's go” The law firm was very thorough with us. It was awesome. I don't want to cry, because I think about and it's amazing that they were able to help me and that we were able to help my son and get the story out there.
- Jay C. Throughout the process, one thing was clear to us, the ultimate interest of our child was the utmost concern of Max and his team and as parents navigating a situation like that, that was refreshing to know we had them firmly on our side. I highly recommend them.