Anesthesia Errors
Anesthesia Errors in Labor And Delivery
A number of factors contribute to labor pains, such as uterine muscle contractions, cervix pressure, stretching of the vagina and birth canal, and pressure of the baby on the bowels and bladder. Commonly used options for pain relief during vaginal delivery include analgesic drugs. In case of a C-section, local, regional, or general anesthesia must be administered.

Anesthesia errors, such as over-dosage of the anesthetic drug, wrong choice of anesthetic technique, failure to monitor the mother and the baby (with fetal heart monitoring and other methods), intubation errors (incorrect tube positioning in the airway or disconnected, overinflated or damaged tube), and communication errors between the anesthesiologist and the rest of the perinatal team can increase the risk of injury to the mother and the baby.
Mistakes in the use of analgesia and anesthesia can put the baby at an increased risk of fetal hypoxia, fetal acidosis, and fetal distress syndrome. In some cases, the adverse outcomes for the baby may include hypoxic-ischemic encephalopathy (HIE), which is a major cause of cerebral palsy.
Analgesia vs. Anesthesia for Childbirth
- Analgesia: Analgesia is used during vaginal delivery to provide relief from labor pain, which is a form of acute pain. Neuraxial labor analgesia, which involves administration of analgesics (pain relievers) as epidural (in the space around the spinal cord), spinal (directly into the spinal cord) or combined spinal-epidural analgesia (CSE), is currently accepted as the most effective technique for pain control during labor and delivery.
- Anesthesia: Unlike analgesia, which numbs the pain without causing a total loss of sensation, anesthesia removes all sensation from the targeted areas. According to the practice guidelines published by the American Society of Anesthesiologists, a spinal block, an epidural or combined anesthesia should be used for most cesarean deliveries. In exceptional cases, general anesthesia may be used (where the mother will be unconscious during the entire surgical procedure).
Regional Anesthesia and the Risks of Instrumental Delivery
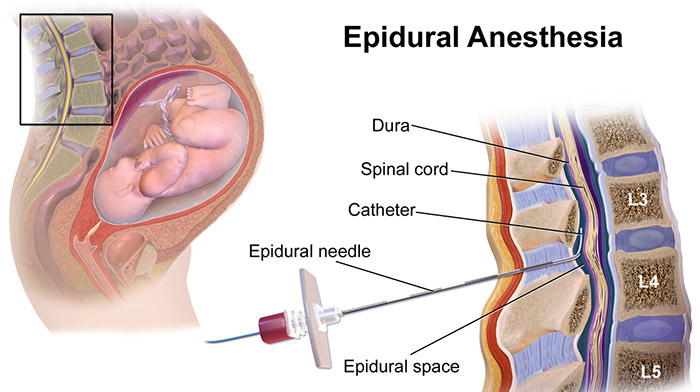
During epidural or spinal anesthesia or analgesia procedure for a vaginal delivery, the anesthesiologist will insert a catheter (a thin tube) underneath the skin tissue into the space around the spinal cord (epidural) or directly into the cerebrospinal fluid (spinal). The catheter will be connected to an infusion pump that delivers the anesthetic continuously until the baby is delivered.
Both epidural and spinal anesthesia have been associated with an increased risk of assisted vaginal delivery (instrumental delivery using forceps or vacuum extractors). This is because it can affect the ability of the mother to “push” during labor and delivery. Randomized clinical trial meta analyses have shown that the use of regional anesthesia prolonged the average duration of labor. At the same time, the rate of instrumental delivery was higher in women receiving spinal or epidural anesthesia (compared to the use of analgesic medications).
A comparison between high-dose epidural and spinal/epidural combination anesthesia showed that the rate of instrumental vaginal delivery was lower when the combination technique was used. Instrument assisted delivery increases the baby’s risk of birth injuries, such as:
- Skull fracture or skull bone displacement
- Cephalohematoma (formation of blood clots underneath the scalp)
- Brain bleeds (intracranial hemorrhage)
- Facial palsy (weakness in the facial muscles)
- Seizures
- Cerebral palsy
Considering the potential adverse outcomes, anesthesiologists administering epidural anesthesia should focus on initiating and maintaining low or altered concentration levels of the pain relief medication to minimize the risk of instrumental vaginal delivery.
Epidural Anesthesia and Prolonged Second Stage of Labor
The first stage of labor is when the cervix is dilated to 10 cm. The second stage of labor is when the baby moves down vaginally, and birth occurs. The third stage (afterbirth) is when the placenta is delivered. Studies have shown that epidural anesthesia or analgesia may be linked to a prolonged second stage of labor in some cases (by up to two hours).
Prolonged labor in the second stage increases the baby’s risk of birth injuries, such as:
- Fetal hypoxia
- Birth asphyxia
- Fetal acidosis
- Fetal bradycardia (low fetal heart rate or FHR)
- Hypoxic ischemic encephalopathy (HIE)
- Cerebral palsy
Considering these potentially serious neonatal outcomes, the anesthesia team and the medial team should work in close coordination to detect early symptoms of fetal distress when epidural anesthesia is administered.
The medical team and the anesthesiologist should also ensure that in case of epidural anesthesia, the woman avoids oral intake of thick liquids and solid foods. (Only clear liquids containing glucose may be allowed).
Oral intake issues should be considered more carefully when the woman has a pre-existing condition, such as obesity or gestational diabetes, or the baby shows signs of respiratory distress syndrome or the electronic fetal heart rate monitor readings are non-reassuring. In these situations, oral intake may increase the risk of cesarean section and/or meconium aspiration syndrome (MAS).
Over-dosage of Anesthetics, Positioning Mistakes and FHR Abnormalities

An excessive dosage of epidural or spinal anesthetic drugs can have direct toxic effects on the baby, and the baby’s toxicity levels may be higher than even the mother’s levels. Potential complications for the baby include abnormal fetal heart rate (FHR) changes, indicating fetal bradycardia or fetal hypoxia. The effects typically occur within the first 30 minutes after the anesthesia is administered through epidural or spinal methods.
Timely drug treatment and maternal change of position may help resolve the condition. In more severe cases of fetal distress, the medical team must be prepared for an emergency cesarean section.
Supine position (lying on the back) when an epidural has been administered may also contribute to maternal hypotension (low blood pressure), increasing the risk of FHR abnormalities and fetal hypoxia. This risk is especially high in heavier expectant mothers. To avoid this risk, the mother should be “wedged” with a positioning device to avoid this drop in blood pressure. The mother and baby should be closely monitored by the anesthesia team and the labor and delivery doctors and nurses for a drop in blood pressure due to being laid flat.
Epidural-Related Maternal Fever and Risks for the Baby
According to research studies, about one in five pregnant women who are administered epidural analgesia or anesthesia may develop an epidural-related fever (above 100.4° F) during labor. This should alert the medical providers to the increased risk for the baby, and the mother should be monitored for maternal fever. The higher the mother’s epidural-induced fever (intrapartum hyperthermia), the greater is the risk of complications for the baby.
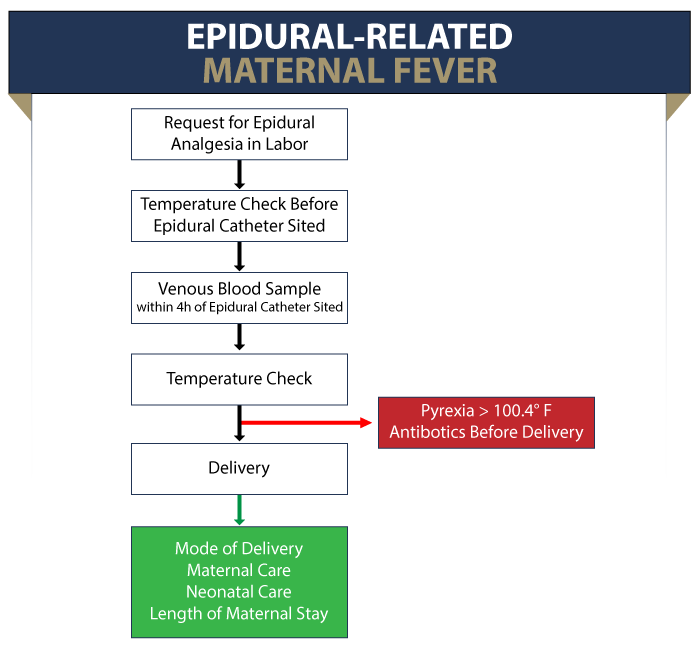
A baby born to a mother with epidural-induced fever should also be evaluated for sepsis (blood infection). Sepsis evaluation will involve invasive tests and baby’s admission to critical care. Antibiotics should be administered until the test results are determined. According to a research study, one out three epidural babies born to first-time mothers received sepsis evaluation compared to one in 10 non-epidural babies.
Research Shows Epidural Hyperthermia may be a Risk Factor for Neonatal Brain Injury
Researchers conducted a meta analysis and systematic review to investigate three questions:
- 1. Can epidural analgesia or anesthesia cause intrapartum hyperthermia (maternal fever)?
- 2. Is maternal fever associated with neonatal brain injury (a spectrum of medical conditions, including HIE and cerebral palsy)?
- 3. Is epidural-induced maternal fever associated with neonatal brain injury?
Researchers analyzed
• 41 studies for question # 1
• 36 studies for question # 2
• Two studies for question # 3
*The analyses showed that epidural anesthesia is indeed associated with maternal fever. Pertaining to this, maternal fever is associated with neonatal brain injury.
Although researchers could not quantify the association between epidural-induced maternal fever and neonatal brain injury, the fact that maternal fever is linked to neonatal brain injury raises questions about whether epidural anesthesia is an independent risk factor of neonatal brain injury.
Anesthesiologists Should Consider the Possibility of Epidural-Induced Fever
A study published in the Lancet journal concluded that there is a progressive rise in maternal temperature of about 33.8 F every 8 hours after the initiation of epidural anesthesia. In other words, epidural-induced fever may depend on the duration of the epidural block.
There is also a possibility that maternal fever during labor may occur because of an underlying chorioamnionitis infection (bacterial infection of the vagina during pregnancy.) As a result, pregnant women are more likely to request epidural anesthesia if they have subclinical (mild and non-observable) chorioamnionitis symptoms, such as uterine tenderness.
In view of this correlation (which is backed by research), anesthesiologists must consider the potential risks of epidural-induced maternal fever while determining the anesthetic drug, dosage, and technique.
Cesarean Delivery & Anesthesia Errors
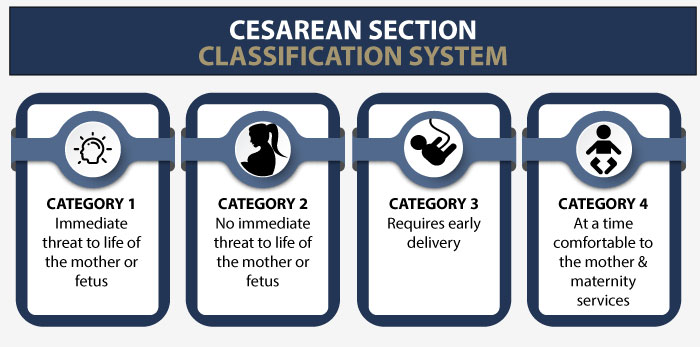
A Cesarean section may be planned in advance or may have to be performed in an emergency. Potential anesthesia errors that can lead to adverse outcomes for the mother and the baby include:
Errors of Dosage
Overdose of epidural or spinal anesthetic during a c-section may lead to consequences, such as cardiac problems or brain damage. On the other hand, under-dosage in case of general anesthesia during c-section may cause the mother to awaken during surgery.
Failure to Monitor Fetal Heart Rate (FHR)
In a scheduled cesarean delivery, the anesthesiologist should determine and document whether the fetal heart rate (FHR) reading is normal before starting anesthesia. In case of an emergency cesarean delivery, continuous fetal heart rate monitoring must be performed to look for any early signs of fetal distress. Failure of the anesthesiologist and the medical team on this front can result in fetal bradycardia, fetal hypoxia, HIE, or cerebral palsy.
Failure to Monitor Other Vital Signs
During a c-section, the anesthesiologist should be present throughout the procedure to monitor the patient’s vital signs and oxygen levels. Failure to notice marked fluctuations in the patient’s breathing, heart rate, and blood pressure levels can have severe consequences for the mother and the baby.
Intubation Errors
In some cases of cesarean section involving general anesthesia (vs. an epidural), an intubation procedure is used where a thin tube is passed into the trachea to facilitate breathing. If the anesthesiologist wrongly places the tube, it can result in breathing complications, mouth lacerations, throat damage, and injuries to the larynx. Common placement mistakes involve the intubation being placed into the esophagus (connecting to the stomach) vs. the trachea (connecting to the lungs). This mistake can be caught if the anesthesiologist is monitoring oxygen and carbon monoxide levels.
Errors of Injection Placement
When the anesthesiologist administers epidural anesthesia, they must place the injection precisely into the epidural space around the spinal cord. In case of spinal anesthesia, the injection must be placed directly into the spinal sac which contains the cerebrospinal fluid. Wrong placement of the injection may not only deprive the patient from pain relief, it may even lead to extreme consequences, such as paralysis.
In some situations, an epidural anesthesia will go up towards the mother’s lungs and heart vs. down and around her pelvis. This is referred to as the epidural being “High”. This is an emergency situation that can place the life and health of both the mother and baby at risk. When this occurs, the proper response is an emergency c-section.
Failure to Review Medical History
The anesthesiologist must review the pregnant woman’s detailed medical chart and history to understand her risks of possible anesthesia complications. They should be aware of her pre-existing medical conditions, current medications, and any known drug allergies. Any errors of omission or commission in this process can create adverse outcomes for the mother and the baby during a c-section.
Delays in Performing Cesarean Delivery
Lack of coordination and poor communication between the anesthesiologist and the labor and delivery team may sometimes result in the doctors waiting too long before an emergency cesarean delivery is performed. Failure to monitor fetal heart rate, attempting other means to induce delivery when a c-section should have been performed, and lack of preparation for an emergency cesarean section are some of the causes of delays in the procedure, which can lead to severe consequences.
Medication Errors Related to Anesthesia
Whether it is a vaginal delivery involving analgesia or a cesarean section requiring anesthesia, medication errors during the administration of anesthesia can pose serious risk to the mother and the baby. Researchers have reported wrong administration of local anesthetics, sedatives and narcotics, muscle relaxants, ketamine, and anticholingerics (drugs to block nerve action) due to a variety of factors, such as:
- Haste
- Inattention
- Fatigue
- Carelessness
- Overtime
- Lack of staff
- Syringe and ampoule swaps
- Inaccurate or confusing syringe labeling
- Incomplete packaging
- Misidentification (sound-alike or look-alike drugs)
- Inaccurate drug dose calculation
- Inexperience or lack of drug knowledge
- Poor communication
Anesthesiologists must be Familiar with Fetal Assessments
Are most anesthesiologists familiar with the implications of abnormal fetal assessments? The anesthesiologist’s lack of understanding about intrapartum fetal assessments may lead to poor anesthetic management, particularly when the baby is experiencing fetal distress. Assessing the fetal health before anesthesia is important because a compromised baby is likely to have poor tolerance to anesthesia.
Lack of familiarity on this front may result in sub-optimal communication between the anesthesiologist and the obstetrics team. A survey carried out in the UK showed that 61% of anesthesiologists claimed they could interpret the readings of electronic fetal heart monitoring (EFHM), yet only 20% of them knew what is the correct range of the baseline FHR (fetal heart rate).

According to the ASA Task Force on Obstetric Anesthesia, “The decision to use a particular anesthetic technique for cesarean delivery should be individualized based on several factors. These include anesthetic, obstetric, or fetal risk factors (for example, elective vs. emergency), the preferences of the patient, and the judgment of the anesthesiologist.”
Is Your Child’s Anesthesia Error Related Complication the Result of Medical Malpractice?
Parents whose children suffer from anesthesia error related complications deserve answers as to how their child developed this condition and whether the complications resulting from it were preventable. Were there signs during the pregnancy, labor, and delivery process that an infection or its related complication was occurring, but appropriate anesthesia administration, correct treatment or an emergency c-section was either delayed or not performed at all? Was a neonatal resuscitation team not called to delivery in a timely manner to address breathing difficulties? Did the baby qualify for hypothermia therapy, but the doctors and nurses failed to perform the appropriate analysis or ignored the results of the analysis?
Our dedicated birth injury lawyers want to help you find those answers and obtain that coveted financial reward necessary to provide care and therapy that can help improve the quality of your child’s life. Winning a lawsuit in this way can improve the quality of your life for a number of reasons.
If your child has been diagnosed with an anesthesia error related injury (including Hypoxic-Ischemic Encephalopathy (HIE) or cerebral palsy), and you suspect this may have been caused in part by medical mistakes, Miller Weisbrod Olesky will thoroughly investigate the facts and hold responsible medical providers accountable by pursuing medical malpractice claims against them. The compensation our clients receive helps them pay for their child’s current and future medical treatment and devices to help the child adjust to living with a permanent disability, and to be able to pay for these cutting-edge devices.
Sometimes families are hesitant to reach out to a medical malpractice attorney or law firm. Other parents feel overwhelmed by their circumstances and worried that they will not be able to help out in a lawsuit involving their child’s birth injury.
Registered Nurses and Nurse-Attorneys Are a Vital Part of Our Birth Injury Team … and Yours

Most national birth injury law firms will employ one or two nurses to assist the review of cases and medical research. But Miller Weisbrod Olesky offers an unmatched number of nurses and nurse-attorney employees support to both the birth injury attorneys and our clients.
Our team of registered nursing staff and nurse-attorneys bring a deep level of medical and personal insight to every client’s case. Our nursing team includes both an experienced labor and delivery nurse as well as an ICU nurse. Working closely with the rest of the team, they investigate the reasons behind a birth injury and how medical professionals breached their standard of care.
Why Should You Talk with the Knowledgeable Attorneys at Miller Weisbrod Olesky?

The only way to find out if you have a birth injury case is to talk to an attorney who understands birth injuries leading to a delay or failure in developmental milestones including birth injuries that cause cerebral palsy. It’s not uncommon that an anesthesia error related complication can be a preventable birth injury, but it takes a detailed expert review of the facts and circumstances of your child’s birth to determine the birth injury was the result of medical malpractice.
At Miller Weisbrod Olesky, a team of committed attorneys, nurses and paraprofessionals uses our detailed medical negligence case review process to assess your potential birth injury case. We start by learning more about you and your child and the status of meeting/missing developmental milestones. Then we gather medical records to determine what happened before, during, and after your delivery. We call in skilled medical experts who review your records and let us know if they think medical errors could have caused your child’s injuries.
If we feel medical negligence caused or contributed to your child’s injuries, we meet with you to discuss how you can receive compensation from the medical professionals who made the errors. Our birth injury attorneys have recovered millions of dollars in settlements for families of babies that have suffered a birth injury.
At no point in our legal intake process will we ask you to pay anything. The medical review of your case and the consultation are free. We only receive payment when you do.
Contact Our National Birth Injury Lawyers
National Birth Injury Law
Our National Birth Injury Attorneys, nurses, and support staff understand that parents of children with birth injuries feel overwhelmed. So, every client has the attention and support of a team of trained, compassionate professionals. But we don’t just offer compassion.
We offer a process to help you discover whether your child’s birth injury, HIE, cerebral palsy or brain injury at birth was caused by medical malpractice.
Call our offices today at (888) 987-0005 for experienced assistance in a free consultation.
Quick Links
Testimonials
- Lyric C. I feel like our voice was heard in a sense of what can possibly go wrong in a delivery and finding us answers. I feel with our settlement, we are now in a comfortable position to provide for our son.
- Lyssa L. They are not just people that say “hey let's get you money and let's go” The law firm was very thorough with us. It was awesome. I don't want to cry, because I think about and it's amazing that they were able to help me and that we were able to help my son and get the story out there.
- Jay C. Throughout the process, one thing was clear to us, the ultimate interest of our child was the utmost concern of Max and his team and as parents navigating a situation like that, that was refreshing to know we had them firmly on our side. I highly recommend them.
Popular Cities
- ★ Dallas Birth Injury
- ★ Houston Birth Injury
- ★ Atlanta Birth Injury
- ★ Chicago Birth Injury
- ★ Philadelphia Birth Injury
Locations
★ Dallas
11551 Forest Central Drive, Ste. 300
Dallas, TX 75243
★ Houston
12929 Gulf Freeway, Ste. 111
Houston, TX 77034