Overventilation and Hypocarbia
Hypocarbia During Birth
Medical professionals can learn more about a newborn’s health status by analyzing their blood. The bloodstream provides a variety of cells, proteins, and gases. This includes levels of oxygen, carbon dioxide, hemoglobin, red blood cell counts, white blood cell counts, and platelet counts.

When blood testing reveals irregularities in the baby’s bloodstream, it can indicate they have birth complication that need quick treatment. These complications can cause or contribute to permanent birth injuries when medical professionals fail to detect or treat them. One of the most significant brain injury risk is hypoxic ischemic encephalopathy (HIE).
HIE is a severe brain injury resulting from a lack of oxygenated blood flowing to the baby’s brain. It can cause neurological damage, delayed developmental milestones, vision impairments, seizures, and other complications. HIE is also the leading cause of cerebral palsy.
When doctors suspect a newborn has HIE at birth, they may provide supplemental oxygenation in the neonatal intensive care unit (NICU). However, sometimes medical professionals improperly set the breathing machine. When the machine over ventilates the baby and removes too much carbon dioxide from their blood, it can cause hypocarbia.

Failing to properly test a newborn’s blood or negligently contributing to their overventilation can worsen their brain damage at birth. When these errors cause hypocarbia and other preventable birth complications, it may be grounds for a medical malpractice lawsuit.
Birth Injury Malpractice Attorneys
Our top rated birth injury attorneys specialize in identifying how medical errors can cause or worsen a child’s birth injuries. If you or someone you know suffered from the effects of overventilation, don’t hesitate to contact our firm. We can answer difficult legal and medical questions and investigate the facts on your behalf.
Free Legal Consultation
Birth Injury Lawyers
(888) 987-0005Our Birth Injury Lawyers are available to meet you in your home or the hospital.
Our vast network of medical experts and in-house nursing staff and nurse-attorneys gives us the edge over our competition. When we take your case, we assign you with an entire medical team. This team not only consists of attorneys but also nursing advocates and medical experts.
Your team is available to assist with any day-to-day treatment you or your child may need. This includes assistance with medical records, scheduling doctors’ appointments, providing transportation, and any other problems that may arise.
We offer all of this on a contingency fee basis. This means you will not pay any fees until after we win your case and secure a settlement. Miller Weisbrod Olesky’s unmatched track record of birth injury results sets us apart from other birth injury law firms.

Recent Birth Injury Settlement:
Birth Injury settlement against a hospital in which nurses and physicians failed to properly monitor the mother's blood pressure during delivery causing an HIE event resulting in neonatal seizures and cerebral palsy at birth. Our team of top-rated birth injury lawyers recovered $13,750,000 for the family to help with future medical expenses and developmental therapy.
What is Hypocarbia?
Hypocarbia (or hypocapnia) is a condition where the baby doesn’t have sufficient levels of carbon dioxide (CO2) in the blood.

Carbon dioxide serves two main purposes within the bloodstream: transporting waste and regulating pH levels. CO2 is a byproduct of cellular respiration; the blood transports it from the body’s tissues to the lungs for exhalation. Inside the blood it appears in the form of bicarbonate, which regulates the body’s acid-base balance.
The body needs sufficient levels of CO2 within the bloodstream to maintain this balance. The proper levels of CO2 in the blood should fall in the range of 35-45 mmHg (millimeters of mercury). When the levels fall below 35 mmHg, it can indicate the baby is in a state of hypocarbia.
What Causes Hypocarbia in Infants?
Hypocarbia can stem from several different issues. One of the main causes is hyperventilation at birth. A baby breathing deeper and more rapidly than normal will expel excess amounts of CO2 with each breath.
Children and adults may hyperventilate when overexerted or anxious, but the causes are much different for newborns. One of the primary causes of rapid and shallow breathing (also known as neonatal tachypnea) is respiratory distress syndrome (RDS).
Respiratory distress syndrome is common in premature births when the baby’s lungs have yet to develop fully. Underdeveloped lungs typically lack a sufficient coating of surfactant. Surfactant is a molecule responsible for increasing airflow in the lungs and preventing the alveoli within the lungs from collapsing.
Lower levels of surfactant will force the baby to breathe harder and faster to take in oxygen. This can drive them into hyperventilation and cause them to expel more CO2 than necessary when exhaling, leading to hypocarbia.
Other pregnancy complications like meconium aspiration syndrome (when fetal waste ends up inside the lungs) can cause respiratory distress. Neonatal infections can also impact breathing, especially when they are severe and develop into rare cases of neonatal sepsis.
Overventilation Leading to Hypocarbia: Causes and Effects
Another common cause of hypocarbia can come from neonatal breathing mismanagement at birth. Children who experience injuries during labor and delivery like hypoxia and birth asphyxia may require specialized breathing treatment upon birth. Depending on the severity of the newborn’s breathing issues, doctors may need to perform neonatal resuscitation.
In other cases, healthcare providers may transfer the infant to the neonatal intensive care unit (NICU). From there, they can hook the baby up to assisted ventilation machine providing supplemental oxygen. These machines can help babies with respiratory distress syndrome and other breathing issues, but improper usage can have adverse effects.

If the ventilation machine is improperly set, the baby can receive too much oxygen and lose an excess amount of CO2 from their bloodstream. This is known as overventilation, and it can have adverse effects on blood flow within the baby’s brain and pH regulation within the body.
Periventricular Leukomalacia (PVL)
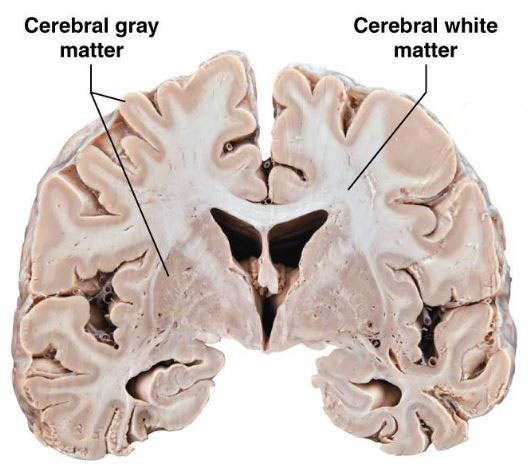
Overventilation can cause hypocarbia as well as lead to periventricular leukomalacia (PVL). This type of brain injury where blood flow cannot reach all parts of the brain. This results in the softening and damage of the white matter tissue around the brain’s ventricles.
PVL can come with symptoms of muscle spasticity and is often an underlying cause of cerebral palsy. Medical professionals must be aware of this risk when administering supplemental oxygen to newborns through ventilation machines.
What Are the Signs of Hypocarbia in Newborns?
Unlike adults who go into hypocarbia, newborns are unable to clearly communicate their symptoms. This is why healthcare providers must learn how to identify signs of the condition as it develops.
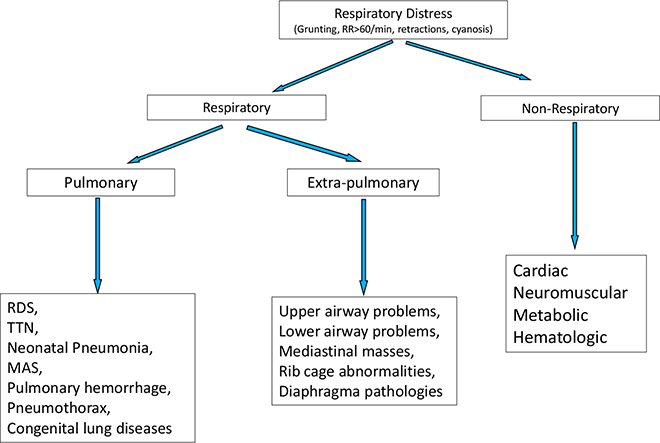
Respiratory Distress Syndrome (RDS)

One of the first signs that may point to an infant’s risk of hypocarbia is having respiratory distress syndrome. A baby in RDS will have rapid, shallow breathing (tachypnea) and a respiratory rate exceeding 60 respirations per minute. Nasal flaring, chest retractions, and grunting are other common signs.
Neonatal Seizures
Due to the electrolyte imbalances from hypocarbia, the baby may start to undergo muscle spasms and cramps. These may escalate into neonatal seizures due to the abnormal electrical activity in the brain. Doctors must keep a watchful eye and prepare to administer anti-convulsant medications in case of an emergency.
Fetal Distress

Monitoring neonatal heart rates can also reveal signs of hypocarbia. Less carbon dioxide in the blood leads to vasoconstriction, meaning the blood vessels contract and decrease blood flow. In response, the baby’s heart rate will decrease with rapid decelerations.
The same will be true in cases of fetal hypocarbia. Fetal heart rate monitoring machines should show decelerations when there is a decrease in CO2 within the unborn baby’s bloodstream. Prolonged decelerations can indicate the baby is in fetal distress and at risk for a brain injury.
There will likely be other symptoms of hypocarbia that the baby will unfortunately have no way of communicating. These can include dizziness, feeling lightheaded, chest tightness, and numbness or tingling around the limbs.
With this in mind, neonatal healthcare providers must pay close attention to the observable signs and symptoms of hypocarbia. They must carefully monitor the baby’s heart rate and breathing patterns, as well as any notable physical or behavioral concerns.
What Are the Possible Complications of Hypocarbia?

Hypocarbia can lead to several different neurological, cardiovascular, and metabolic complications.
Among the most serious complications of hypocarbia are brain injuries like periventricular leukomalacia (PVL) and hypoxic ischemic encephalopathy (HIE). These injuries form because of vasoconstriction, preventing oxygenated blood from flowing to the brain and other parts of the body.
Prolonged hypocarbia and vasoconstriction can also lead to organ dysfunction, particularly to the heart. When prolonged, it reduces the myocardial oxygen supply and leads to hypoxemia (reduction of oxygen in the blood).
Carbon dioxide is slightly acidic, so a CO2 deficiency in the blood can throw off the body’s pH balance. This can cause a complication known as respiratory alkalosis, when the body’s blood pH rises above 7.45.
Respiratory alkalosis can affect calcium levels in the blood, leading to hypocalcemia and related muscle spasms. It can also cause lower phosphate and potassium levels, which can contribute to muscle weakness and fatigue.
How to Diagnose and Treat Hypocarbia?
When doctors suspect hypocarbia, they should order an arterial blood gas (ABG) test to measure CO2 levels and pH balance. A bicarbonate test (also known as a CO2 blood test) is another common test for measuring CO2 levels.

An arterial blood gas test will reveal the amount of partial pressure of carbon dioxide (PaCO2) within the arterial blood. This is a measure of how much CO2 has already dissolved in the blood.
A normal range for PaCO2 levels is between 35-45 mmHg (millimeters of mercury). When an infant’s readings fall below 35 mmHg, it is a sign of hypocarbia.
Additionally, imaging tools like X-rays and CT scans can reveal any possible complications that are causing the baby’s respiratory distress. leading to hyperventilation and thus developing hypocarbia. Examples of conditions these scans can reveal include pneumonia, pulmonary edema, or other diseases of the lungs.
Mechanical ventilation can be both a cause and a treatment option for hypocarbia.

When a baby requires assisted ventilation via respiratory machines, it is critical medical professionals understand how to use them.
If the baby begins to show signs of overventilation, healthcare providers must quickly adjust the settings. They may need to decrease the peak pressure or modify tidal volumes (the amount of air delivered with each breath). In some cases, they may need to change the mode on the ventilator.
Sometimes neonatal infections like pneumonia or sepsis contribute to a baby’s hyperventilation and subsequent hypocarbia. In these cases, doctors must quickly administer antibiotic medications to restore proper CO2 and oxygen levels.
Hypocarbia can lead to a brain injury relatively quickly due to its effects on restricting blood flow. It’s important healthcare providers quickly order blood testing and administer treatment to prevent damage to the baby's brain.
How to Prevent Hypocarbia?
Not all cases of hypocarbia are preventable, but there are actions healthcare providers can take to mitigate the risk.
Prenatal Testing

Like with all birth injury prevention, careful monitoring throughout the mother’s pregnancy and delivery is key to catching potential complications. This begins with proper prenatal testing and managing any of the mother’s pregnancy complications that may affect the baby’s blood CO2 levels, such as a maternal infection.
Continued Fetal and Neonatal Monitoring
Throughout pregnancy and during labor, medical providers should look for sudden changes in fetal status using heart rate monitoring. This can help them catch any labor and delivery complications before the baby goes into fetal distress.
Upon birth, healthcare professionals should continue close physical examination of the baby’s breathing and overall appearance. Metrics like the APGAR score can indicate to doctors when the baby may need neonatal resuscitation and further respiratory intervention.
Proper training on how ventilation machines work can help healthcare professionals avoid errors that can lead to over ventilation brain injuries.
Did Medical Negligence Cause My Child’s Hypocarbia?

Brain injuries like periventricular leukomalacia and hypoxic ischemic encephalopathy can permanently alter a baby’s life trajectory. When these injuries occur because of hypocarbia from overventilation or another form of neonatal breathing mismanagement, it constitutes medical malpractice.
If a family believes medical negligence caused or worsened a child’s injuries, legal support may be an option. A specialized birth injury attorney can review the medical records and circumstances to assess whether a claim exists.
Families who have experienced the effects of overventilation errors deserve to know whether better medical care could have prevented them. Our top rated birth injury lawyers will help you find those answers and obtain the necessary funds to secure treatment.
Our team will thoroughly investigate the facts, holding responsible parties accountable by pursuing medical malpractice claims.
What is the Statute of Limitations in a Birth Injury Lawsuit?
A statute of limitations (SOL) is a law that sets a time limit on how long an injured person has to file a lawsuit after an accident. It is essential to understand that statutes of limitations vary based on the case and the state where you file. For instance, the deadline for birth injury claims is typically different from other claims, such as injury to private property.
Generally, the clock starts ticking on the date the injury occurred. However, there are exceptions to this rule. In some cases, the statute of limitations starts when a person discovers or reasonably should have discovered an injury. When dealing with government agencies, SOLs can become even more complex.
For example, if the party that injured you was:
- A federal employee
- Employed by a military hospital, Veterans Administration facility, or a federally funded medical entity
You may need to file a birth injury claim under the Federal Tort Claims Act (FTCA). In FTCA cases, claimants must go through certain administrative procedures before filing a lawsuit. In some states, you may have less time to give notice if:
- The negligent party was a local or state government hospital.
- The doctors and medical providers are employees of a governmental entity.
If you file your case outside of the statute of limitations, the court will typically dismiss it. This means you will not be eligible to recover compensation for you or your child’s injuries.
Determining when a statute of limitations begins on your case can be tricky. If you are considering pursuing compensation for a birth injury, contact an attorney as soon as possible.
How Can Our Birth Injury Attorneys Help?

Brain injuries from overventilation are preventable with proper medical care. However, it takes an expert review of the facts of your birth to determine whether medical professionals made preventable errors.
Our Process
Our national team of committed birth injury attorneys, nurses and paraprofessionals works to answer these questions and seek compensation. We use our detailed medical negligence case review process to assess your potential birth injury case.
We start by learning more about your pregnancy by gathering records to determine what happened during and after your delivery. This includes a detailed review of the treatment doctors provided or failed to provide in the neonatal intensive care unit.
We will call in skilled medical experts who review your records and provide insight into where medical professionals went wrong. If we feel medical negligence caused or worsened you or your child’s injuries, we meet with you to discuss further.
At no point in our legal intake process will we ask you to pay anything. The medical review of your case and the consultation are free. We only receive payment once you do. The sooner you reach out, the sooner we can investigate your case and gather the evidence to support your claim.
We work on a contingency fee basis, meaning you will not pay any legal fees until we win your case. We do not purse any medical malpractice cases unless we fully believe we can win.
Contact us today to schedule your free consultation by calling our toll-free line at (888) 987-0005. You can also reach us by filling out our online request form.
National Birth Injury Law
Our National Birth Injury Attorneys, nurses, and support staff understand that parents of children with birth injuries feel overwhelmed. So, every client has the attention and support of a team of trained, compassionate professionals. But we don’t just offer compassion.
We offer a process to help you discover whether your child’s birth injury, HIE, cerebral palsy or brain injury at birth was caused by medical malpractice.
Call our offices today at (888) 987-0005 for experienced assistance in a free consultation.
Quick Links
Testimonials
- Lyric C. I feel like our voice was heard in a sense of what can possibly go wrong in a delivery and finding us answers. I feel with our settlement, we are now in a comfortable position to provide for our son.
- Lyssa L. They are not just people that say “hey let's get you money and let's go” The law firm was very thorough with us. It was awesome. I don't want to cry, because I think about and it's amazing that they were able to help me and that we were able to help my son and get the story out there.
- Jay C. Throughout the process, one thing was clear to us, the ultimate interest of our child was the utmost concern of Max and his team and as parents navigating a situation like that, that was refreshing to know we had them firmly on our side. I highly recommend them.
Popular Cities
- ★ Dallas Birth Injury
- ★ Houston Birth Injury
- ★ Atlanta Birth Injury
- ★ Chicago Birth Injury
- ★ Philadelphia Birth Injury
Locations
★ Dallas
11551 Forest Central Drive, Ste. 300
Dallas, TX 75243
★ Houston
12929 Gulf Freeway, Ste. 111
Houston, TX 77034