Intrauterine Growth Restriction
What Is Placental Insufficiency?
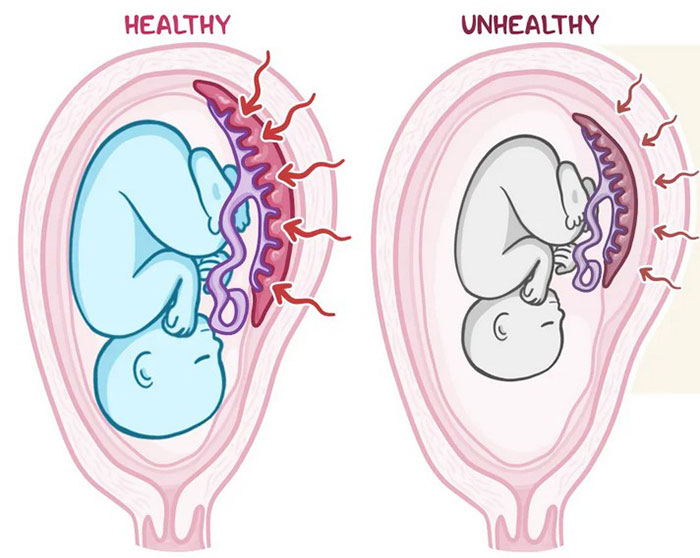
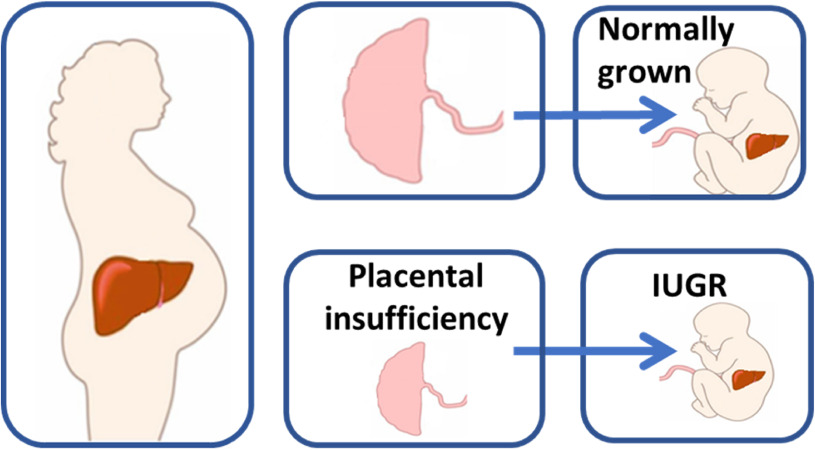
Placental insufficiency is a pregnancy complication in which oxygen and vital nutrients are not properly delivered to the fetus. This increases the risk of Intrauterine growth restriction (IUGR). Intrauterine growth restriction (IUGR) or "Fetal Growth Restriction" means the baby’s size is abnormally small, which can cause serious complications around the time of birth as well as long-term stunted growth.
Both Placental insufficiency and IUGR increase the risks of birth complications for the baby including hypoxic-ischemic encephalopathy (HIE), which is the leading cause of cerebral palsy.
Early diagnosis of placental insufficiency can help obstetricians and nurses prepare for potential birth complications and plan steps that will reduce the chances of a birth injury. A diagnosis of placental insufficiency requires Doppler ultrasound exams and a careful evaluation of medical history. The incidence of placental insufficiency is fairly high occurring in about 10% of all pregnancies.
While conservative treatment options such as medications and antioxidants may be considered, an early scheduled cesarean section delivery is typically recommended in these cases.
Diagnosing IUGR
To detect placental insufficiency, the medical provider should perform a thorough physical exam of the expectant mother and review her detailed medical history. Periodic Doppler ultrasound screenings can help in early diagnosis of the condition. MRI imaging will also provide valuable information to make a more conclusive diagnosis of placental insufficiency.
Any placental abnormality, such as obstructed blood supply and hemorrhages (bleeds), which indicate a higher risk of placental insufficiency can be identified with MRI films. If the expectant mother is diagnosed with oligohydramnios (low amniotic fluid for the gestational age) placental insufficiency should be suspected, and more regular Doppler studies and MRI tests should be performed.
When placental insufficiency is suspected, continuous fetal heart rate monitoring at well-mother checkups and during labor must be performed to detect signs of fetal distress. Detection of any placental abnormality should serve as the first clinical indicator to the medical provider that the baby is not receiving optimal levels of oxygen and nutrients, which may restrict fetal growth (diagnosed as IUGR).
Although advancements in obstetric monitoring technologies have increased the likelihood of early detection of placental insufficiency and IUGR pregnancy, according to researchers up to 50% of the IUGR cases remain undiagnosed, and are either first recognized at birth or very late in the pregnancy. As a result, pregnancy audits show that a large number of cases of preventable stillbirth are related with the medical failure to detect SGA (small for gestational age) before birth.
Testing the Health of the Baby with IUGR
When IUGR is diagnosed or suspected, a close monitoring of the baby is necessary for the rest of the pregnancy, during labor and immediately after birth. Prior to delivery, if the test results show potential fetal distress, medical providers should prepare for emergency cesarean section.
Tests during this period should include:
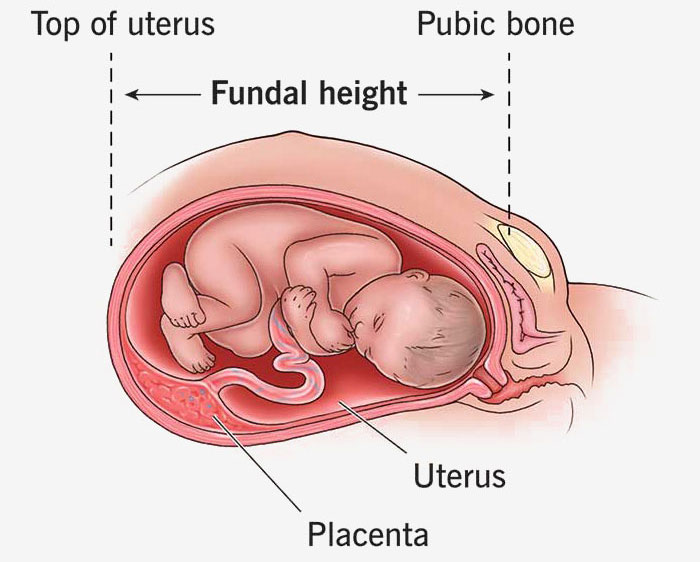
- Body weight evaluation of the mother during every prenatal visit. If the weight gain is below the expected range for the gestational age, the medical provider should be alert to the possibility of fetal growth restriction.
- Non-Stress Tests (NSTs) should be performed to track how the in-utero baby’s heart responds to various types of physical stimulation and movements.
- Biophysical Profile (BPP) is a combination of tests to measure fetal breathing, fetal muscle tone, fetal movement and amniotic fluid volume to predict the risk of severe fetal hypoxia, HIE (which may lead to cerebral palsy), and death.
- Fetal Heart Rate Monitoring (FHR) can contribute to the timely detection of early-onset IUGR because of the higher variability in heart rate detected in growth-restricted babies compared to healthy unborn babies.
- Doppler Velocimetry is different from the regular Doppler ultrasound that assesses the baby’s heartbeat. Doppler velocimetry test can check whether the baby’s blood supply is restricted (causing insufficient oxygen and nutrient supply) and whether the baby is anemic, growing slowly or has a low amniotic fluid index (oligohydramnios).
What are the Types of Fetal Growth Restriction?
Intrauterine Growth Restriction (IUGR) is classified into two types: early-onset IUGR and late-onset IUGR. This reflects the gestational age of the baby when IUGR is diagnosed.
Early-Onset IUGR
When fetal growth restriction is detected before 32 weeks of pregnancy, it is called “early-onset IUGR”. This is a more severe condition, associated with significant placental insufficiency, often leading to severe fetal hypoxia. Premature birth is more likely for babies with this early-onset IUGR, and they are at an increased risk of conditions such as hypoxic-ischemic encephalopathy, which may lead to cerebral palsy, or even death in some cases.
Late-Onset IUGR
When fetal growth restriction is detected during or later than 32 weeks of pregnancy, it is called late-onset IUGR. It’s usually associated with placental insufficiency of a milder degree. However, even though the placental disruption is relatively mild, babies with late-onset IUGR are at an increased risk of rapid deterioration of their health and fetal distress. Close monitoring with electronic fetal monitoring and other exams is critical to minimizing birth complications and birth injuries.

Managing IUGR for Improved Outcomes
Unfortunately, both antenatal (before birth) and postnatal (after birth) therapies continue to be an area of clinical research and currently there is no confirmed treatment for IUGR. Conservatively, the use of low-dose aspirin, vitamin C, vitamin E, and antioxidants may be considered in an attempt to improve placental function in cases of IUGR.
The anticoagulant heparin, which is used to prevent blood clotting, may be administered to treat placental insufficiency because of its known properties to fight apoptosis (cellular death) and lowering of inflammation. At the same time, heparin may indirectly work as a growth factor to improve placentation.
In most cases, a planned or emergency cesarean section delivery is the most viable option in a pregnancy severely affected by placental insufficiency and fetal growth restriction. The delivery will usually take place preterm (before 36 weeks), which further increases the risks for the baby. If the medical provider decides to wait and prolong the pregnancy to allow further development of the baby, they must couple the delay with very close monitoring of the in-utero baby along with readiness to perform an emergency c-section at any time.
IUGR and Cerebral Palsy
According to several research studies, babies with IUGR are five to seven times more likely to develop cerebral palsy. Reduced oxygen supply to the developing brain during pregnancy can put the baby at an increased risk of hypoxic-ischemic encephalopathy, leading to cerebral palsy and other neurodevelopmental disabilities. White matter injury patterns in the brain are also seen in some babies with IUGR, which causes cerebral palsy.
Moreover, babies with IUGR are at an increased risk of lung and heart abnormalities, such as bronchopulmonary dysplasia (BPD, a chronic lung disease affecting newborns) and pulmonary hypertension (a type of blood pressure affecting the lungs and heart). Therefore, it is critical that a neonatal resuscitation team be present at the delivery of babies diagnosed with IUGR to assist with any breathing complications at birth.
Neonatologists, pediatricians and NICU nurses must exercise caution in how they conduct neonatal resuscitation in babies with IUGR. For an oxygen-deprived IUGR baby, if they are suddenly exposed to excessive amounts of oxygen, it may cause hyperoxia (oxygen toxicity). Hyperoxia can result in white matter damage, leading to cerebral palsy. Therefore, medical providers must be careful to provide the correct amount of oxygen during the resuscitation, but not over-oxygenate babies with this birth complication.
Is Your Child’s Birth Injury the Result of Medical Malpractice?
Parents whose children suffer from placental insufficiency and IUGR related birth injuries or birth complications want and deserve answers as to cause of their child’s injury and whether mistakes by the doctors and nurses contributed to the injury.
- Were there signs of IUGR during the pregnancy, labor, and delivery process, or presence of risk factors, which were either not recognized or properly treated?
- Did the medical team fail to order a series of tests to diagnose IUGR in a timely manner?
- Was the decision to perform a cesarean delivery delayed?
- During the labor and delivery, were there clear indications that their baby was suffering from fetal distress, but appropriate actions were not taken by the obstetrician or nurses?
- Did the neonatal resuscitation team delay in providing important breathing support after birth?
- Were serious neonatal conditions like hypoglycemia or jaundice missed or treated incorrectly?
- Should brain cooling (also called “hypothermia therapy”) have been offered to your baby, but the doctors and nurses failed to perform the appropriate tests or ignored the results of the tests?
The focused and confident birth injury lawyers at Miller Weisbrod Olesky, who have been through the legal minefields before, will help you determine if mistakes of the medical providers caused a birth injury to your child, including Hypoxic-Ischemic Encephalopathy (HIE) or cerebral palsy. Our profound and proven birth injury attorneys have represented families all over the United States in their time of need after a birth injury. We use our experience and expertise to obtain you and your child a medical malpractice settlement that will help provide specialized medical therapy to maximize the quality of life and independence of your child throughout their life.
Sometimes families are reluctant to contact a medical malpractice lawyer. It’s also not uncommon for parents to feel overwhelmed by the responsibilities they encounter in caring for their injured child and worried that they will not be able to help out in a lawsuit involving their child’s birth injury. Our birth injury attorneys and nursing staff will address these hesitations and concerns, so you can focus on your child and maximizing their care.
Registered Nurses and Nurse-Attorneys Are a Vital Part of Our Birth Injury Team…and Yours

Most birth injury law firms will employ one or two nurses to assist the review of cases and medical research. But Miller Weisbrod Olesky offers an unmatched number of nurses and nurse-attorney employees support to both the birth injury attorneys and our clients.
Our team of registered nursing staff and nurse-attorneys bring a deep level of medical and personal insight to every client’s case. Our nursing team includes both an experienced labor and delivery nurse as well as an ICU nurse. Working closely with the rest of the team, they investigate the reasons behind a birth injury and how medical professionals breached their standard of care.
Why Should You Talk with the Knowledgeable Attorneys at Miller Weisbrod Olesky?

The only way to find out if you have a birth injury case is to talk to a lawyer experienced in birth injury lawsuits. It’s not uncommon that a birth related complication results in a preventable birth injury, including cerebral palsy, but it takes a detailed expert review by a birth injury attorney of the medical records from your child’s birth to determine if the birth injury was the result of medical malpractice.
At Miller Weisbrod Olesky, a team of committed lawyers, nurses and paralegals uses our detailed medical negligence case review process to assess your child’s potential birth injury case. We start by learning more about you and your child and the status of meeting/missing developmental milestones. Then we gather medical records to determine what happened before, during, and after your delivery. We call in skilled medical experts who review your records and let us know if they think medical errors could have caused your child’s injuries.
If we feel medical negligence caused or contributed to your child’s injuries, we meet with you to discuss how you can receive compensation from the medical professionals who made the errors. Our birth injury attorneys have recovered millions of dollars in settlements for families of children that have suffered a birth injury.
At no point in our legal intake process will we ask you to pay anything. The medical review of your case and the consultation are free. We only receive payment when you do.
Contact Our Birth Injury Lawyers
National Birth Injury Law
Our National Birth Injury Attorneys, nurses, and support staff understand that parents of children with birth injuries feel overwhelmed. So, every client has the attention and support of a team of trained, compassionate professionals. But we don’t just offer compassion.
We offer a process to help you discover whether your child’s birth injury, HIE, cerebral palsy or brain injury at birth was caused by medical malpractice.
Call our offices today at (888) 987-0005 for experienced assistance in a free consultation.
Quick Links
Testimonials
- Lyric C. I feel like our voice was heard in a sense of what can possibly go wrong in a delivery and finding us answers. I feel with our settlement, we are now in a comfortable position to provide for our son.
- Lyssa L. They are not just people that say “hey let's get you money and let's go” The law firm was very thorough with us. It was awesome. I don't want to cry, because I think about and it's amazing that they were able to help me and that we were able to help my son and get the story out there.
- Jay C. Throughout the process, one thing was clear to us, the ultimate interest of our child was the utmost concern of Max and his team and as parents navigating a situation like that, that was refreshing to know we had them firmly on our side. I highly recommend them.
Popular Cities
- ★ Dallas Birth Injury
- ★ Houston Birth Injury
- ★ Atlanta Birth Injury
- ★ Chicago Birth Injury
- ★ Philadelphia Birth Injury
Locations
★ Dallas
11551 Forest Central Drive, Ste. 300
Dallas, TX 75243
★ Houston
12929 Gulf Freeway, Ste. 111
Houston, TX 77034