Gestational Diabetes
What is Gestational Diabetes?
Pregnancy is almost always accompanied by some degree of "insulin resistance" because of the placental secretion of certain hormones. Insulin is the body’s hormone that allows glucose (i.e. sugar) to leave the blood stream and enter the cells of our muscles, fat and liver to produce energy for our body. Insulin resistance occurs when the cells in our muscles, fat and liver do not respond well to insulin therefore leaving more glucose in the blood vs. pulling it out to create energy. If insulin resistance is high enough and glucose (sugar) levels are too high in the blood stream this is a condition defined as “diabetes”.

Gestational diabetes or maternal diabetes, clinically known as Gestational Diabetes Mellitus (GDM), occurs in pregnant women when their pancreatic function is inadequate to overcome the pregnancy-related insulin resistance and glucose levels in the blood reach certain levels.
This is usually a condition that occurs just during the pregnancy and is not a permanent after delivery of the baby. But there are several risk factors to the mother and baby that accompany gestational diabetes.
GDM increases the risk of preeclampsia (maternal hypertension disorder). Consequences for the babies may include fetal macrosomia (large for gestational age), fetal hypoglycemia (low blood sugar), respiratory distress, birth defects, prolonged delivery due to the large baby, cephalopelvic disproportion, fetal distress and birth injury. According to the American Diabetes Association, nearly one in 10 pregnancies is affected by gestational diabetes. Timely diagnosis and management of this condition can help prevent potentially severe outcomes for the baby’s health.
What are Signs of Gestational Diabetes
Medical providers should identify the risk factors as well as look for the early signs of gestational diabetes so that appropriate steps can be taken to manage it and protect the mother and baby’s health. While any woman during pregnancy may develop gestational diabetes, the following risk factors indicate a higher likelihood of developing this condition:
- Overweight: Having a body mass index (BMI) of at least 30 at the time of getting pregnant.
- Older age: The risk of GDM increases with age, and women above the age of 25 to 30 are generally at a higher risk.
- Family history: The risk increases when diabetes runs in the family,and in particular, if any immediate relatives have it.
- GDM history: Having gestational diabetes in a previous pregnancy increases the risk of getting it again in a subsequent pregnancy.
- Pre-diabetes diagnosis: Mild elevation of blood sugar levels detected prior to the pregnancy should be seen as a risk factor for GDM.
- Bed rest advice: Women who are advised bed rest during pregnancy may have a higher risk of GDM due to restricted levels of activity.
- Medical history: Pre-existing medical conditions, such as hypertension, PCOS, metabolic syndrome, and heart disease are risk factors for gestational diabetes.
- Carrying multiple babies: Pregnancy with multiples could increase the mother’s risk for gestational diabetes.
- Ethnicity: Women of African American, American Indian, Hispanic, Asian American, and Pacific Islander descent may be at a higher risk.
How Do You Test for Gestational Diabetes?

Nine out of 10 pregnant women in the US are likely to have at least one risk factor for Gestational Diabetes Mellitus (GDM). Considering this fact, it is best to adopt a universal screening approach to diagnose this condition. GDM generally occurs around the 24th week of pregnancy (second trimester), so the testing will be performed anywhere between 24th and 28th week. Medical providers should test earlier, if the risk of developing gestational diabetes is higher.
Some of the early signs and symptoms that women experiencing GDM or pre-GDM include: unusual hunger or thirst, frequent urination, blurred vision, fatigue, and loss of weight despite eating more are some of the signs that may indicate gestational diabetes.
The condition can be diagnosed using the following blood tests:
Glucose Screening Test
This test measures the blood sugar level at the time of testing. The mother will drink a liquid containing glucose, and after a gap of one hour, her blood sample will be taken to check the level of blood sugar. A glucose or blood sugar result of up to 140 mg/dL (milligrams per deciliter or one-tenth of a liter) is considered normal. If the measurement shows a blood sugar level above 140 mg/dL, a second test called glucose tolerance test must be administered.
Glucose Tolerance Test
This test is designed to determine a pregnant woman’s blood sugar levels before and after she drinks a liquid containing glucose.
- Step 1: The mother will undergo overnight fasting (not eating) prior to the test. A blood sample is drawn to measure the blood sugar fasting level.
- Step 2: The mother drinks the liquid containing glucose, and the blood sugar level is measured at intervals of one hour, two hours, and in some cases, three hours afterward.
The normal fasting blood glucose level at one hour is up to 180 mg/dL, at two hours is up to 155 mg/dL, and at three hours is up to 140 mg/dL. If any of these measurements is found to be higher than normal, the test should be repeated after four weeks. If two or more of the test results show higher than normal readings, the gestational diabetes diagnosis should be confirmed.
Gestational Diabetes Complications for the Baby
Overt gestational diabetes mellitus may adversely impact the baby’s in-utero development and the complications put the baby at much higher risk for birth injury. In the first trimester, major birth defects or spontaneous abortions may be induced. In the second and third trimesters, the babies of mothers with GDM are vulnerable to fetal macrosomia (excessive fetal growth), fetal hypoglycemia, respiratory distress, and other common causes of birth injury.
Stillbirth
Stillbirth refers to the loss of a baby during or after the 20th week of pregnancy (prior to that, it is called miscarriage). According to the National Library of Medicine, stillbirth or fetal death is more likely after 35 weeks in pregnant women who are diagnosed with gestational diabetes.
While the precise cause of stillbirths occurring with GDM remains unknown, it’s observed that the baby’s development in the uterus may slow down because of poor blood flow, blood vessel damage, or high blood pressure in women with poor blood sugar control.
A research study conducted by the University of Manchester and the University of Leeds showed that failure to diagnose gestational diabetes mellitus significantly increases the risk of stillbirth. The researchers compared the symptoms of gestational diabetes and care standards of 291 women who had a stillbirth to another group of 733 women who did not have a stillbirth.
The researchers found that pregnant women with signs of GDM who remained undiagnosed had a four times higher risk of stillbirth than those who were diagnosed. The risk steadily increased with increasing content of glucose in the blood. Researchers determined that the increased risk of stillbirth was eliminated with appropriate GDM screening tests and diagnosis.
Dr. Tomasina Stacey, the lead author of the study (which was published in BJOG: An International Journal of Obstetrics and Gynecology) said: “The good news is that women with gestational diabetes have no increase in stillbirth risk if national guidelines are followed for screening, diagnosis, and management. The bad news is that the guidelines are not always followed, and some women therefore experience avoidably higher risk.”
Birth Defects

When a pregnant woman is diagnosed with gestational diabetes, the medical providers should be alert to the possibility of birth defects. The risk of major birth defects is higher in the first trimester of pregnancy in these cases. The medical team should watch out for potential birth defects in the brain and spine, heart, and blood vessels, kidneys and urinary system, and the digestive system.
Research has shown the toxic effects of maternal diabetes mellitus on embryo development and the increased risk of congenital malformations. In women with pregestational diabetes (PGDM), the risk of fetal structural defects may be three to four times higher compared to women with non-diabetic pregnancy.
Diabetic embryopathy (congenital mal-developments related to gestational diabetes) may adversely affect the baby’s developing organ systems, such as the skeletal system, central nervous system, cardiovascular system, renal system, and gastrointestinal system.
A research study conducted by the Stanford University School of Medicine and Stanford Children’s Health and published in JAMA Pediatrics showed that moderately elevated levels of blood glucose in pregnancy are correlated to congenital heart defects in babies – even when the blood glucose is below the cutoff for gestational diabetes.
According to the study’s lead author and pediatric cardiologist Dr. James Priest, it was already known that babies born to diabetic mothers are at an increased risk of having congenital heart disease. But with this new research, it is now established that even when a pregnant woman does not meet the clinical criteria for GDM diagnosis, the risk of fetal heart disease still exists if her blood glucose values are elevated.
In this study, the researchers evaluated the blood glucose levels of two groups of women during the 2nd trimester of pregnancy. One group of 180 women carried babies without congenital heart disease, while the other group included 55 women whose babies had tetralogy of fallot (a structural heart defect, which causes blue baby syndrome, with the baby receiving too little oxygen).
Researchers found that the average blood sugar levels were higher in women carrying babies with tetralogy of fallot compared to the women in the control group. Dr. Priest commented on the findings that most of the times doctors have little idea of what may have caused a fetal heart defect. This research study sheds important light on this issue.
Fetal Macrosomia
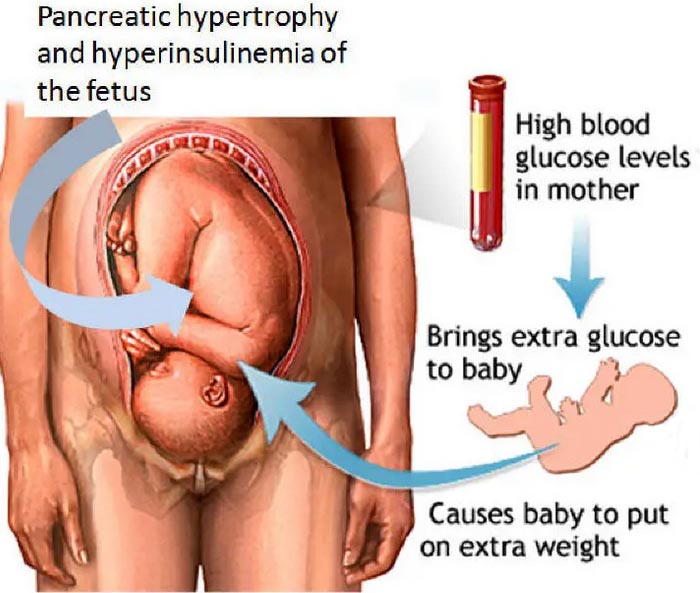
When a baby is large for their gestational age (LGA), the condition is called fetal macrosomia. The fetus obtains its entire nutrition from maternal blood. But when the mother’s blood contains excessive glucose, the baby’s pancreas starts producing more insulin and converts the excess glucose to fat. Consequently, large amounts of fat deposits lead to an oversized fetus.
If the birth weight of the baby exceeds 9 pounds, the condition is termed as fetal macrosomia. According to researchers, about 15 to 45 percent of the babies born to women with GDM may have macrosomia. This is a common adverse outcome of gestational diabetes mellitus if it is undiagnosed and untreated in time.
Babies with macrosomia are at an increased risk of clavicle fractures (broken collarbone), shoulder dystocia (baby’s shoulders are stuck during vaginal delivery, increasing the risk of brain damage, nerve damage, and arm or collarbone fracture), and brachial plexus injury (when the baby’s neck is stretched to one side during delivery). The risk of Erb’s palsy (nerve damage resulting in loss of muscle function in the shoulder and arm) is also higher in macrosomic babies.
Babies with macrosomia are at an increased risk for labor and delivery complications that can lead to birth injuries including clavicle fractures (broken collarbone), shoulder dystocia (baby’s shoulders are stuck during vaginal delivery, increasing the risk of brain damage, nerve damage, and arm or collarbone fracture), and brachial plexus injury (when the baby’s neck is stretched to one side during delivery). The risk of Erb’s palsy (nerve damage resulting in loss of muscle function in the shoulder and arm) is also higher in macrosomic babies. Almost all of these pregnancy complications can be avoided by careful screening and the willingness to recommend and perform cesarean section and when necessary due to evidence of fetal distress or prolonged labor an emergency c-section.
Babies with macrosomia have a five times higher risk of developing severe hypoglycemia (low blood sugar) and twice the risk of neonatal jaundice compared to non-diabetic mothers. Both of these neonatal birth injuries can be avoided with careful screening and aggressive treatment.
Neonatal Hypoglycemia

When the baby is diagnosed with low blood sugar levels right after delivery, the condition is termed as hypoglycemia. One of the causes of neonatal hypoglycemia when the blood glucose levels of the mother have been consistently high during pregnancy, resulting high insulin levels in the fetus. If the baby’s insulin levels continue to be elevated after delivery this can cause hypoglycemia.
This leads to an abnormally low level of blood sugar in the baby. Medical providers should check this level immediately after childbirth and, if necessary, they should administer glucose through IV. During labor and delivery, it is essential to monitor the blood sugar levels very closely. Depending on the condition, the medical team may give insulin to the mother to keep her blood glucose level in control so that the baby’s blood sugar does not suddenly drop to dangerously low levels after delivery.
This leads to an abnormally low level of blood sugar in the baby. Medical providers should check this level immediately after childbirth in babies born to mothers suffering from gestational diabetes. If the levels are low, the doctors and nurses should treat immediately including the administration of glucose through IV.
During labor and delivery, it is essential to monitor the blood sugar levels very closely. Depending on the condition, the medical team may give insulin to the mother to keep her blood glucose level in control so that the baby’s blood sugar does not suddenly drop to dangerously low levels after delivery.
Postnatal hypoglycemia is considered the most critical metabolic complication in babies born to mothers with gestational diabetes. Research has shown that if hypoglycemia is the baby remains undiagnosed and unrecognized neonatal hypoglycemia can often result in a brain injury including hypoxic-ischemic encephalopathy.
Screening for neonatal hypoglycemia is mandatory for all infants from diabetic mothers (IDMs) from the first hour life – no matter what may be the type and severity of maternal diabetes, and whether the baby’s presentation at birth appears to be initially fine. The incidence of hypoglycemia in infants born to diabetic mothers may be as high as 40 percent.
Hypoglycemic episodes in babies can continue for up to a week after birth. The National Guideline on Neonatal Hypoglycemia Screening suggests that babies born to mothers with gestational diabetes mellitus should be screened immediately after delivery, and then at intervals of 30 minutes, one hour, two hours, four hours, eight hours, 12 hours, and at any other time when symptoms of low blood sugar may appear.
In addition, screening must be performed 30 minutes after the start of glucose IV therapy, and after every significant adjustment to the glucose dosage. A rapid response with glucose therapy in babies showing signs of hypoglycemia can prevent the occurrence of long-term neurological lesions. Medical providers should always anticipate neonatal hypoglycemia when the mother has gestational diabetes and start screening the baby from the first moments of childbirth – irrespective of whether or not any clinical symptoms are present.
Respiratory Distress Syndrome
Excessive glucose concentration and too much insulin in the baby’s system can hamper the full and normal development of the lungs. This may result in respiratory distress (troubled breathing), especially in preterm babies born before the 37th week of pregnancy. But even in general, gestational diabetes mellitus in the mother predisposes the baby to respiratory distress syndrome.
A New England Journal of Medicine study found a strong correlation between GDM and respiratory distress syndrome in babies. Researchers examined data pertaining to one group of 10,152 babies of non-diabetes mothers and another group of 805 babies of mothers with gestational diabetes. Respiratory distress syndrome was found in 1.3 percent babies in the non-diabetic group, while in the diabetic group 23.4 percent (nearly one in four) babies had the syndrome.
Another retrospective study also found that gestational diabetes is associated with an increased respiratory morbidity in babies. The researchers, moreover, have not been able to determine the underlying cause of this relationship between gestational diabetes and respiratory morbidity in infants. Hyperinsulinemia and poor glycemic control of the baby as well as an increased possibility of a caesarian section in these cases may contribute to a higher risk of neonatal respiratory distress. If not promptly treated, respiratory distress can cause a birth injury to the brain including hypoxic-ischemic encephalopathy that can lead to cerebral palsy.
Is Your Child’s Maternal Diabetes Related Complication the Result of Medical Malpractice?
Parents whose children suffer from gestational diabetes related complications as well as parents who have suffered the loss of their baby due to these complications deserve an answer to how their child developed this condition and whether the complications resulting from it were preventable. Whether the injury occurred during delivery or in the neonatal period, families are entitled to compensation for mistakes in handling babies of a diabetic mother.
If your child has been diagnosed with gestational diabetes related injury, and you suspect this may have been caused in part by medical mistakes, Miller Weisbrod Olesky will thoroughly investigate the facts and hold responsible medical providers accountable by pursuing medical malpractice claims against them. The compensation our clients receive helps them pay for their child’s current and future medical treatment and devices to help the child adjust to living with a permanent disability, and to be able to pay for these cutting edge treatments.
Sometimes families are hesitant to reach out to a medical malpractice attorney or law firm. Other parents feel overwhelmed by their circumstances and worried that they will not be able to help out in a lawsuit involving their child’s birth injury.
Why Should You Talk with the Knowledgeable Attorneys at Miller Weisbrod Olesky?

The only way to find out if you have a birth injury case is to talk to an attorney who understands birth injuries leading to a delay or failure in developmental milestones including birth injuries that cause cerebral palsy. Many times a gestational diabetes related complication is a preventable birth injury, but it takes a detailed expert review of the facts and circumstances of your child’s birth to determine the birth injury was the result of medical malpractice.
At Miller Weisbrod Olesky, a team of committed attorneys, nurses and paraprofessionals uses our detailed medical negligence case review process to assess your potential birth injury case. We start by learning more about you and your child and the status of meeting/missing developmental milestones. Then we gather medical records to determine what happened before, during, and after your delivery. We call in skilled medical experts who review your records and let us know if they think medical errors could have caused your child’s injuries.
If we feel medical negligence caused or contributed to your child’s injuries, we meet with you to discuss how you can receive compensation from the medical professionals who made the errors.
At no point in our legal intake process will we ask you to pay anything. The medical review of your case and the consultation are free. We only receive payment when you do.
Contact Our National Birth Injury Lawyers
National Birth Injury Law
Our National Birth Injury Attorneys, nurses, and support staff understand that parents of children with birth injuries feel overwhelmed. So, every client has the attention and support of a team of trained, compassionate professionals. But we don’t just offer compassion.
We offer a process to help you discover whether your child’s birth injury, HIE, cerebral palsy or brain injury at birth was caused by medical malpractice.
Call our offices today at (888) 987-0005 for experienced assistance in a free consultation.
Quick Links
Testimonials
- Lyric C. I feel like our voice was heard in a sense of what can possibly go wrong in a delivery and finding us answers. I feel with our settlement, we are now in a comfortable position to provide for our son.
- Lyssa L. They are not just people that say “hey let's get you money and let's go” The law firm was very thorough with us. It was awesome. I don't want to cry, because I think about and it's amazing that they were able to help me and that we were able to help my son and get the story out there.
- Jay C. Throughout the process, one thing was clear to us, the ultimate interest of our child was the utmost concern of Max and his team and as parents navigating a situation like that, that was refreshing to know we had them firmly on our side. I highly recommend them.
Popular Cities
- ★ Dallas Birth Injury
- ★ Houston Birth Injury
- ★ Atlanta Birth Injury
- ★ Chicago Birth Injury
- ★ Philadelphia Birth Injury
Locations
★ Dallas
11551 Forest Central Drive, Ste. 300
Dallas, TX 75243
★ Houston
12929 Gulf Freeway, Ste. 111
Houston, TX 77034