Uterine Atony
Uterine Atony Complications
Labor is strenuous on both the mother’s and baby’s bodies. OB-GYNs, nurses, and all other medical professionals must be prepared to treat any possible labor and delivery complications that arise in the process. However, maternal complications like uterine atony can sometimes happen after the baby is already born.

Uterine atony occurs when the uterus fails to contract after delivery, and when left untreated, or insufficiently treated, it can cause excessive bleeding that threatens the mother’s life. Globally, it is one of the leading causes of maternal mortality.
Healthcare providers must understand and be alert to the signs of uterine atony and the methods for treating it. When they make negligent errors that worsen a mother’s injuries or result in her untimely death, it can constitute medical malpractice.
Birth Injury Malpractice Attorneys
Our top-rated birth injury attorneys specialize in identifying mismanaged labor and delivery complications. If you or someone you know suffered from the effects of uterine atony, don’t hesitate to contact our firm. We can answer difficult legal and medical questions and investigate the facts on your behalf.
Free Legal Consultation
Birth Injury Lawyers
(888) 987-0005Our Birth Injury Lawyers are available to meet you in your home or the hospital.
Our vast network of medical experts and in-house nursing staff and nurse-attorneys gives us the edge over our competition. When we take your case, we assign you with an entire medical team. This team not only consists of attorneys but also nursing advocates and medical experts.
Your team is available to assist with any day-to-day treatment you or your child may need. This includes assistance with medical records, scheduling doctors’ appointments, providing transportation, and any other problems that may arise.
We offer all of this on a contingency fee basis. This means you will not pay any fees until after we win your case and secure a settlement. Miller Weisbrod Olesky’s unmatched track record of birth injury results sets us apart from other birth injury law firms.

Recent Birth Injury Settlement:
Birth Injury settlement against a hospital in which nurses and physicians failed to properly monitor the mother's blood pressure during delivery causing an HIE event resulting in neonatal seizures and cerebral palsy at birth. Our team of top-rated birth injury lawyers recovered $13,750,000 for the family to help with future medical expenses and developmental therapy.
What is Uterine Atony?
Uterine atony (also known as uterine hypotonicity) is a complication where the mother’s uterus fails to contract after delivering the baby. While it can also affect contractions during childbirth, uterine atony primarily affects the afterbirth process of delivering the placenta.
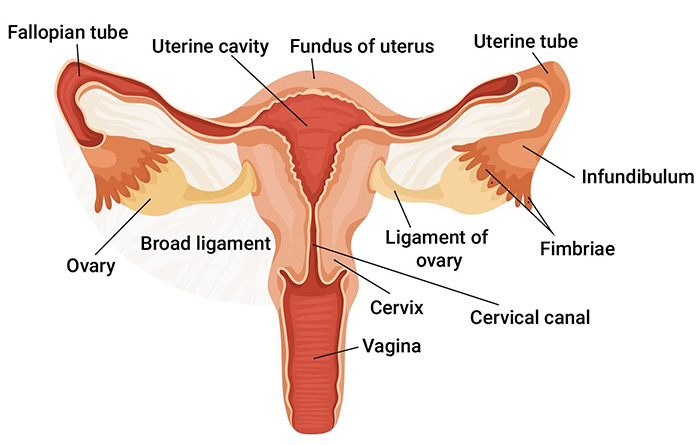
The uterus is a hollow, muscular organ that holds and nourishes unborn babies. The organ itself has three layers:
- Endometrium –the inner, epithelial layer
- Myometrium – the smooth, muscle layer
- Perimetrium – the serosal outer surface of the uterus
The uterus naturally tightens (or contracts) during labor to force the baby out of her womb through the birth canal. The mother’s body should continue to stimulate mild contractions after the baby is born to deliver her placenta, a temporary organ that develops in the uterus during pregnancy to provide the fetus with blood, oxygen and nutrients.
After delivery, blood vessels in the uterus break open to allow the placenta to detach from the uterine lining. With uterine atony, the muscles of the myometrium soften and weaken to the point where they cannot compress those open blood vessels with contractions. This leaves the blood vessels exposed and results in vaginal bleeding known as postpartum hemorrhaging.
Uterine atony can happen in both vaginal births and C-section deliveries. It’s estimated to occur in around 2% of all deliveries in the United States.
Not all cases of atony result in postpartum hemorrhaging, but healthcare providers must be prepared for that possibility. If uterine atony does result in postpartum hemorrhaging, it is considered a medical emergency and requires immediate intervention.
What Causes Uterine Atony?
There can be multiple reasons why the uterus fails to contract both during labor and afterward. This can include uterine deformities and previous surgical procedures for injuries such as a uterine rupture. However, there are often multiple factors that work together to result in the complication.
How Does Oxytocin Cause Uterine Atony?
The main cause of uterine atony is when the uterus does not adequately respond to the oxytocin hormone.
A woman’s body makes oxytocin throughout her lifetime, with increased production during pregnancy. As the fetus presses against her cervix, it triggers a nerve impulse that sends a message to the pituitary gland in her brain to produce more oxytocin. The oxytocin travels to her uterus to stimulate contractions.
Sometimes the mother may have a hormone imbalance that causes a deficiency in oxytocin, which will typically result in a prolonged or arrested labor. For women with these issues, their doctors may prescribe medications to induce labor. The most common is Pitocin, which is a synthesized version of oxytocin.
Doctors typically give Pitocin intravenously when inducing a woman whose labor has not started, but it is also given to women in labor whose contractions need to be strengthened for their labor to progress.
Pitocin can be effective in inducing labor, but issues can occur when doctors prescribe too high of a dosage. The mother’s uterine muscle receptors sometimes become desensitized to the chemical after too much time on it.
Or in other cases, too high of a dose for too long can overstimulate the uterus and cause contractions that are too frequent and too forceful (a condition known as uterine hyperstimulation). This can result in the uterus’s natural relaxation and re-contraction cycles being thrown off, which can weaken blood vessel compression after birth.
What are Risk Factors for Uterine Atony?
Other factors and characteristics of a mother’s pregnancy and labor can increase the risk for uterine atony, including:
- Uterine Overdistension: When the uterus is overdistended (meaning overly inflated or pushed out), it can weaken the effectiveness of contractions during labor and afterward.
There can be numerous causes for uterine overdistension. Examples of complications that cause it include macrosomia, polyhydramnios, twin labor, uterine fibroids, or chorioamnionitis. - Prolonged or Spontaneous Labor: Labor that is either too long or too short can be a risk factor for uterine atony. Prolonged labor can indicate that a mother’s contractions are too weak to push out the child, which can foreshadow similar issues with delivering the placenta during afterbirth.
Additionally, precipitous labor (labor lasting under three hours) can be a risk factor for atony because the uterus may not have enough time to properly contract and clamp the open blood vessels in the uterine wall post-delivery. - Maternal Obesity: Expecting mothers with a BMI of 30 or higher are at an increased risk for pregnancy complications like gestational diabetes and preeclampsia. Doctors may prescribe a medication called magnesium sulfate to manage these complications (particularly preeclampsia).
Magnesium sulfate can inhibit muscle contraction, which can include affecting uterine contractions and increase her risk of experiencing atony. - General Anesthesia: When general anesthesia is used on the mother during labor and delivery, the anesthetic agents may impact the uterine muscles and limit their ability to respond to hormones like oxytocin.
Other risk factors may include a mother’s previous history of experiencing uterine atony. Her healthcare provider must ask for her medical history and inquire about any complications from previous pregnancies to better understand her risk.
If an expecting mother exhibits two or more of these known risk factors, labor and delivery teams should make preparations and have a treatment plan ready in the event she experiences uterine atony. Failing to prepare where risk is clearly identifiable may be grounds for medical malpractice when it results in an injury.
What are the Signs of Uterine Atony?
The biggest sign of uterine atony is excessive bleeding coming from the uterus after delivery. While postpartum vaginal bleeding is normal, heavy bleeding typically indicates a larger issue. OB-GYNs and other medical professionals should be able discern between normal bleeding and a concerning amount of bleeding.
As the mother sustains significant blood loss, her blood pressure levels will also lower, and her heart rate will increase. Healthcare providers should keep an eye on both metrics after delivery to monitor for any sudden drops or increases.

Visibly, the mother may begin to look pale and report feeling dizzy or faint. In cases of severe blood loss, she may even lose consciousness. Healthcare providers should also be alert if she discloses feeling any lower back pain or is unable to urinate.
What are the Complications of Uterine Atony?
The most concerning complication of uterine atony is postpartum hemorrhaging because of the threat it poses to the mother’s life. The American College of Obstetricians and Gynecologists listed postpartum hemorrhaging as one of the leading causes of maternal mortality and morbidity worldwide.
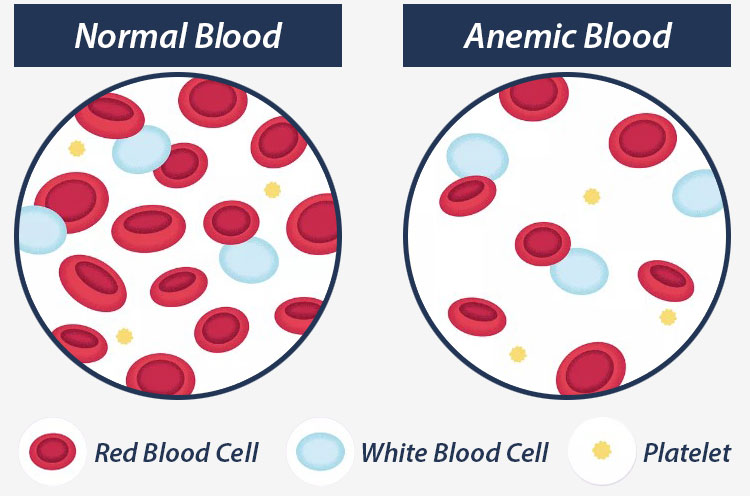
In some cases, postpartum hemorrhaging can cause anemia in mothers due to the loss of significant red blood cells.
Other blood disorders can occur after postpartum hemorrhaging in addition to anemia. Examples include hypovolemic shock and disseminated intravascular coagulation, a condition causing blood clots to form throughout the body.
While rare, hypovolemic shock can result from excessive blood loss and prevent oxygen from reaching the heart, liver, and kidneys.
This complication can be very dangerous for the mother, but it is only possible when more than 20% of her blood volume is lost. This is unlikely to occur in cases of uterine atony but is possible, especially in situations where medical professionals miss the early signs to intervene.
It’s important to note that most women who experience uterine atony end up making a full recovery. However, if a mother plans to have future pregnancies, her risk increases for experiencing uterine atony a second time.
How is Uterine Atony Diagnosed?

Healthcare providers can suspect uterine atony by tracking the mother’s blood loss after delivery. They may do this by weighing or keeping count of the number of pads and sponges they use to absorb her blood.
If the amount of blood loss is concerning, doctors will likely opt to perform a vaginal examination. The medical professional will place one hand on the mother’s abdomen and insert the other hand inside her vagina to feel the size and softness of her uterus.
Doctors will also examine the mother’s vagina, cervix and uterus to see if there are any tears or lacerations contributing to the blood loss. They will also check for any retained placental tissue.
Alongside a physical examination, doctors should track the mother’s heart rate and blood pressure. They may order a series of blood tests to monitor her red blood cell count and blood clotting factor. These tests are to check for any related complications like anemia or disseminated intravascular coagulation.
How to Treat Uterine Atony?

The immediate goal when managing a mother’s uterine atony is to stop the bleeding as fast as possible, and then to replace the lost blood and fluids. Doctors will need to apply pressure to the uterine walls to manually compress the blood vessels and stop the bleeding.
There are several ways to do this: they may decide to pack the mother’s uterus with medical gauze, or in more severe cases they can perform a medical procedure known as a balloon tamponade. This involves inserting a balloon into the mother’s uterus and then inflating it to maintain pressure against the uterine lining.
Administering medication is another possible treatment method. If not tried already, medical professionals may decide to administer Pitocin or Cytotec to induce contractions to deliver the placenta. Other medications, such as Methylergonovine, can be used to control uterine bleeding.
If these options are not possible or prove to be ineffective, doctors may need to perform surgery. There are a couple of different types of procedures to stop postpartum hemorrhaging, with the most common being uterine curettage. This involves scraping the retained blood and placental tissue from the uterus.
Uterine artery ligation is also sometimes performed to stop postpartum hemorrhage from uterine atony. This procedure involves tying off the blood vessels in the uterus to stop bleeding using surgical sutures.
If uterine curettage and artery ligation are not possible or ineffective, the “last resort” procedure is a hysterectomy, where the mother’s entire uterus is removed. This will eliminate the mother’s chances of future pregnancies, but doctors may deem it necessary if they cannot stop the bleeding and her life is at risk.
After the surgery is completed or the bleeding has been stopped another way, the mother will likely require IV fluids. If she has lost a significant amount of blood, a blood transfusion may be needed to supplement her low blood count.
Can Uterine Atony be Prevented?
There is no way to completely prevent a mother from experiencing uterine atony. However, healthcare providers can assess her risk using known information about her pregnancy and medical history.
They can prepare for possible medical intervention by having access to medications like Pitocin and having additional help and equipment.
Did Doctors Mismanage My Post-Delivery Complication?

Uterine atony is a serious maternal complication that can have fatal outcomes, but the vast majority of mothers survive it and fully recover. However, this favorable prognosis is dependent on competent medical care.
Birth injury negligence, such as missing risk factors or surgical errors when operating, can lead to a mother’s preventable injuries. If a family believes medical negligence worsened a mother’s injuries or caused her death, legal support may be an option. A specialized birth injury attorney can review the medical records and circumstances to assess whether a claim exists.
Families who have experienced the effects of postpartum injuries deserve to know whether better medical care could have prevented them. Our top rated birth injury lawyers will help you find those answers and obtain the necessary funds to secure treatment.
Our team at Miller Weisbrod Olesky will thoroughly investigate the facts, holding responsible parties accountable by pursuing medical malpractice claims.
What is the Statute of Limitations in a Birth Injury Lawsuit?
A statute of limitations (SOL) is a law that sets a time limit on how long an injured person has to file a lawsuit after an accident. It is essential to understand that statutes of limitations vary based on the type of case and the state where it is filed. For instance, the deadline for birth injury claims is typically different from other claims, such as injury to personal property, fraud, contract disputes, and collection of debts.
Generally, the clock starts ticking on the date the injury occurred. However, there are exceptions to this rule, and in some cases, the statute of limitations starts when a person discovers or reasonably should have discovered an injury.
When dealing with government agencies, SOLs can become even more complex.
For example, if the party that injured you was:
- A federal employee
- Employed by a military hospital, Veterans Administration facility, or a federally funded medical entity
You may need to file a birth injury claim under the Federal Tort Claims Act (FTCA). In FTCA cases, claimants must go through certain administrative procedures before filing a lawsuit. In some states, if the negligent party was a local or state government hospital or the doctors and medical providers are employees of a governmental entity, the time period in which you must give "notice" may be shorter.
If your case is filed outside of the statute of limitations, it will typically be dismissed, and you will not be eligible to recover compensation for your injuries. Determining when a statute of limitations begins on your case can be tricky. If you're considering pursuing compensation for a birth injury, contacting an attorney as soon as possible is in your best interest.
How Can Birth Injury Attorneys at Miller Weisbrod Olesky Help?

Labor and delivery complications are not always preventable, but medical errors are. It takes an expert review of the facts of your birth to determine whether medical professionals mismanaged your uterine atony.
Our Process
At Miller Weisbrod Olesky, our team of committed birth injury attorneys, nurses and paraprofessionals works to answer these questions and seek compensation. We use our detailed medical negligence case review process to assess your potential birth injury case.
We start by learning more about your pregnancy by gathering records to determine what happened during and after your delivery. This includes a detailed review of the treatment doctors provided or failed to provide after labor.
We will call in skilled medical experts who review your records and provide insight into where medical professionals went wrong. If we feel medical negligence caused or worsened your postpartum injuries, we meet with you to discuss further.
At no point in our legal intake process will we ask you to pay anything. The medical review of your case and the consultation are free. We only receive payment once you do. The sooner you reach out, the sooner we can investigate your case and gather the evidence to support your claim.
We work on a contingency fee basis, meaning you will not pay any legal fees until we win your case. We do not purse any medical malpractice cases unless we fully believe we can win. Contact us today to schedule your free consultation by calling our toll-free line at (888) 987-0005. You can also reach us by filling out our online request form.
National Birth Injury Law
Our National Birth Injury Attorneys, nurses, and support staff understand that parents of children with birth injuries feel overwhelmed. So, every client has the attention and support of a team of trained, compassionate professionals. But we don’t just offer compassion.
We offer a process to help you discover whether your child’s birth injury, HIE, cerebral palsy or brain injury at birth was caused by medical malpractice.
Call our offices today at (888) 987-0005 for experienced assistance in a free consultation.
Quick Links
Testimonials
- Lyric C. I feel like our voice was heard in a sense of what can possibly go wrong in a delivery and finding us answers. I feel with our settlement, we are now in a comfortable position to provide for our son.
- Lyssa L. They are not just people that say “hey let's get you money and let's go” The law firm was very thorough with us. It was awesome. I don't want to cry, because I think about and it's amazing that they were able to help me and that we were able to help my son and get the story out there.
- Jay C. Throughout the process, one thing was clear to us, the ultimate interest of our child was the utmost concern of Max and his team and as parents navigating a situation like that, that was refreshing to know we had them firmly on our side. I highly recommend them.
Popular Cities
- ★ Dallas Birth Injury
- ★ Houston Birth Injury
- ★ Atlanta Birth Injury
- ★ Chicago Birth Injury
- ★ Philadelphia Birth Injury
Locations
★ Dallas
11551 Forest Central Drive, Ste. 300
Dallas, TX 75243
★ Houston
12929 Gulf Freeway, Ste. 111
Houston, TX 77034