Respiratory Distress Syndrome
What is Respiratory Distress Syndrome?
Respiratory Distress Syndrome (RDS) is a birth complication that involves a serious breathing problem that may occur in premature babies whose lungs are not fully developed. Babies born before 28 weeks of gestation are at a particularly high risk of RDS, but the condition may also affect full-term babies. An estimated seven percent of all newborns will suffer from respiratory distress syndrome birth complication.

Medical interventions, such as oxygenation and ventilation are usually required. When the risk of premature birth is high, the medical providers should consider corticosteroids administration as a preventative measure to the expectant mother between 24 and 34 weeks of gestation. The medical team should also be prepared to provide timely neonatal resuscitation according to the updated guidelines to babies born with RDS.
Failure to recognize the risk factors for RDS or respond to RDS after birth with appropriate neonatal resuscitation can lead to a birth injury including a brain injury like hypoxic ischemic encephalopathy (HIE) which is a leading cause of cerebral palsy.
What Causes Neonatal RDS?
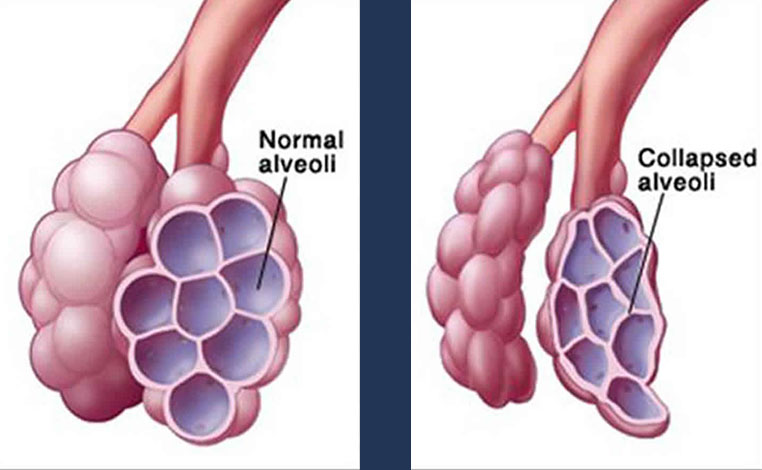
Respiratory distress syndrome in babies primarily occurs due to the deficiency of surfactant in the lungs. Surfactant is a slippery liquid present in fully developed lungs, which increases the airflow in lungs and prevents the air sacs from collapsing with deflation. Surfactant is produced in the baby’s lungs at about 26 weeks of gestation. As the fetal growth progresses, the lungs produce higher volumes of surfactant.
The small air sacs in the baby’s lungs are coated with surfactant to prevent them from collapsing. As the air sacs open, the oxygen enters the bloodstream from the lungs, while carbon dioxide from the bloodstream goes into the lungs. In preterm babies, the lack of surfactant can cause the air sacs to deflate, leading to respiratory distress syndrome.
The doctors like obstetricians and labor and delivery/neonatal nurses should recognize the risk factors of RDS so that they can diagnose and treat the condition early. Risk factors include:
- Induction of labor or cesarean section before the baby is full-term
- Birth complications that reduce the blood flow to the baby
- Rapid labor
- Baby is sick at the time of birth
- Hypothermia (baby is unable to keep body temperature warm at the time birth)
- Maternal diabetes
- Maternal infection
- Twins or multiple pregnancy
- A sibling was born with a RDS birth complication
What are Symptoms of RDS?
Babies with respiratory distress syndrome may show the following signs and symptoms:
- Rapid breathing (tachypnea) right after birth
- Grunting sound accompanies each breath
- Flaring (widening) nostrils with each breath
- Bluish tone or changing color of the baby’s lips, toes, and fingers
- Chest retractions (inward pull of the muscles between the ribs and breastbone when breathing)
Recognizing these signs and symptoms of RDS by the neonatal medical team is critical to initiating quick treatment in order to prevent RDS from leading to a hypoxic or anoxic brain injury to the baby.
Diagnosing Neonatal RDS
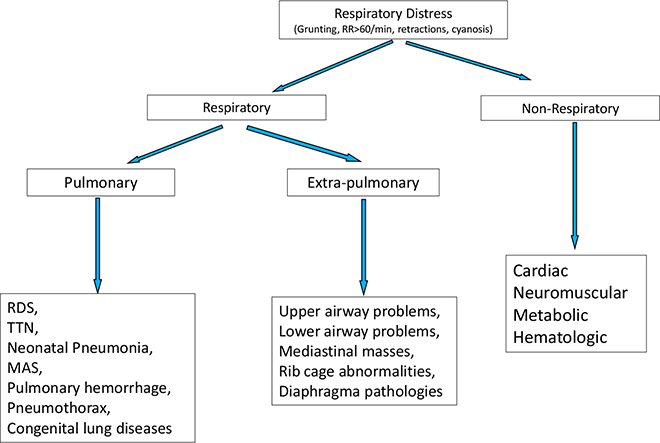
Babies with respiratory distress syndrome will usually exhibit signs of tachypnea (fast breathing) with a respiratory rate exceeding 60 respirations per minute. Nasal flaring, chest retractions, and grunting are other common signs. The initial evaluation should include a thorough physical examination and medical history.
The medical team should monitor the baby’s vital signs, use a pulse oximeter to determine oxygen saturation, and perform blood gas testing. Medical tests may include:
- Chest radiography to determine the functioning of the lungs and heart
- Blood, tracheal aspirate, and cerebrospinal fluid cultures
- Blood tests to rule out an infection
- Blood gas tests to determine if the baby has sufficient oxygen in the blood
- Echocardiogram and other heart tests to identify potential congenital heart defects
RDS Treatments

Babies with respiratory distress syndrome may be treated with neonatal resuscitation using non-invasive techniques and respiratory support. The medical team can provide oxygen via nasal CPAP (continuous positive airway pressure), nasal cannula, bag/mask, or oxygen hood. In more severe cases, intubation and ventilator support is usually required.
Surfactant therapy through intubation followed by nasal CPAP is now increasingly used. The baby should be screened for congenital heart defects after 24 hours. It is equally important to focus on any other possible causes of RDS in premature babies, such as infection.
It is critical that these neonatal resuscitation interventions take place quickly to avoid a hypoxic or anoxic brain injury. Failure to quickly initiate such treatment is often considered medical malpractice if the delay results in an unnecessary birth injury such as HIE or cerebral palsy.
Complications Associated with RDS
Delayed diagnosis or improper treatment for neonatal RDS may lead to a number of life-threatening complications, such as:
- Intraventricular hemorrhage or IVH (brain bleeds in the ventricles)
- Intracranial hemorrhage (bleeds between the brain tissue and skull)
- Periventricular leuckomalacia (cerebral white matter injury)
- Hypoxic Ischemic Encephalopathy (HIE)
- Bronchopulmonary dysplasia or BPD (chronic lung disease)
- Pneumothorax (air leaks into the chest cavity from the lungs)
- Atelectasis (lung collapse)
- Sepsis (blood infection)
- Vision impairment
- Intellectual disability
- Cerebral palsy
How to Prevent RDS in Babies?
Prevention of neonatal respiratory distress syndrome largely boils down to prevention of preterm birth and administration of proper treatment when preterm birth is unavoidable. Proper monitoring and care during pregnancy is vital so that the risk of premature birth is identified, and appropriate medical interventions are made.
When premature birth is imminent via labor induction or cesarean section, medical providers should perform 3D ultrasound exams and other lab tests to assess fetal lung maturity. After carefully weighing the risks of delaying preterm birth versus the risk of RDS, the medical team can make the best decision.
When preterm delivery between 24 and 34 weeks of gestation is necessary, the medical providers should consider administering corticosteroid therapy to promote the baby’s lung development and sufficient production of surfactant. Two doses of betamethasone 12 mg or four doses of dexamethasone 6 mg may be delivered to the mother at least 48 hours prior to delivery in order to induce surfactant production in the baby’s lungs.
In absence of corticosteroid therapy during pregnancy, prophylactic surfactant therapy may be administered to the premature baby who is at a high risk of developing respiratory distress syndrome. Studies have shown that surfactant therapy given through the trachea (intratracheal) may reduce the risk of severe lung complications and neonatal death.
Is Your Child’s Birth Injury the Result of Medical Malpractice?
Parents whose children suffer from respiratory distress syndrome related birth injuries or birth complications want and deserve answers as to the cause of their child’s injury and whether mistakes by the doctors and nurses contributed to the injury.
- Were there signs of birth injuries or birth complications during the pregnancy, labor, and delivery process, or presence of risk factors, which were either not recognized or properly treated?
- Did your baby require corticosteroids prior to birth, but the treatment was not given or improperly given.
- During the labor and delivery, were there clear indications that their baby was suffering from fetal distress, but appropriate actions were not taken by the obstetrician or nurses?
- Did the medical team fail to order a series of tests to diagnose the condition in a timely manner?
- Was the decision to perform a cesarean delivery delayed?
- Did the neonatal resuscitation team delay in providing important breathing support?
- Should brain cooling (also called “hypothermia therapy”) have been offered to your baby, but the doctors and nurses failed to perform the appropriate tests or ignored the results of the tests?
Our national birth injury attorneys that have seen the unfortunate birth complications due to the failure to diagnose and treat RDS have extensive experience in this and all areas of birth injury medical malpractice. The lawyers and nurses at Miller Weisbrod Olesky will help you determine if mistakes of the medical providers caused a birth injury to your child, including Hypoxic-Ischemic Encephalopathy (HIE) or cerebral palsy.
Our award-winning birth injury attorneys have represented families all over the United States in their time of need after a birth injury. We use our experience and expertise to obtain for you and your child a medical malpractice settlement that will help provide specialized medical therapy in order to maximize the quality of life and independence of your child throughout their life.
Sometimes families are reluctant to contact a medical malpractice lawyer. It’s also not uncommon for parents to feel overwhelmed by the responsibilities they encounter in caring for their injured child and worried that they will not be able to help out in a lawsuit involving their child’s birth injury. Our birth injury attorneys and nursing staff will address these hesitations and concerns, so you can focus on your child and maximizing their care.
Registered Nurses and Nurse-Attorneys Are a Vital Part of Our Birth Injury Team…and Yours

Most birth injury law firms will employ one or two nurses to assist the review of cases and medical research. But Miller Weisbrod Olesky offers an unmatched number of nurses and nurse-attorney employees support to both the birth injury attorneys and our clients.
Our team of registered nursing staff and nurse-attorneys bring a deep level of medical and personal insight to every client’s case. Our nursing team includes both an experienced labor and delivery nurse as well as an ICU nurse. Working closely with the rest of the team, they investigate the reasons behind a birth injury and how medical professionals breached their standard of care.
Why Should You Talk with the Knowledgeable Attorneys at Miller Weisbrod Olesky?

The only way to find out if you have a birth injury case is to talk to a lawyer experienced in birth injury lawsuits. It’s not uncommon that a birth related complication results in a preventable birth injury, including cerebral palsy, but it takes a detailed expert review by a birth injury attorney of the medical records from your child’s birth to determine if the birth injury was the result of medical malpractice.
At Miller Weisbrod Olesky, a team of committed lawyers, nurses and paralegals uses our detailed medical negligence case review process to assess your child’s potential birth injury case. We start by learning more about you and your child and the status of meeting/missing developmental milestones. Then we gather medical records to determine what happened before, during, and after your delivery. We call in skilled medical experts who review your records and let us know if they think medical errors could have caused your child’s injuries.
If we feel medical negligence caused or contributed to your child’s injuries, we meet with you to discuss how you can receive compensation from the medical professionals who made the errors. Our birth injury attorneys have recovered millions of dollars in settlements for families of children that have suffered a birth injury.
At no point in our legal intake process will we ask you to pay anything. The medical review of your case and the consultation are free. We only receive payment when you do.
Contact Our Birth Injury Lawyers
National Birth Injury Law
Our National Birth Injury Attorneys, nurses, and support staff understand that parents of children with birth injuries feel overwhelmed. So, every client has the attention and support of a team of trained, compassionate professionals. But we don’t just offer compassion.
We offer a process to help you discover whether your child’s birth injury, HIE, cerebral palsy or brain injury at birth was caused by medical malpractice.
Call our offices today at (888) 987-0005 for experienced assistance in a free consultation.
Quick Links
Testimonials
- Lyric C. I feel like our voice was heard in a sense of what can possibly go wrong in a delivery and finding us answers. I feel with our settlement, we are now in a comfortable position to provide for our son.
- Lyssa L. They are not just people that say “hey let's get you money and let's go” The law firm was very thorough with us. It was awesome. I don't want to cry, because I think about and it's amazing that they were able to help me and that we were able to help my son and get the story out there.
- Jay C. Throughout the process, one thing was clear to us, the ultimate interest of our child was the utmost concern of Max and his team and as parents navigating a situation like that, that was refreshing to know we had them firmly on our side. I highly recommend them.
Popular Cities
- ★ Dallas Birth Injury
- ★ Houston Birth Injury
- ★ Atlanta Birth Injury
- ★ Chicago Birth Injury
- ★ Philadelphia Birth Injury
Locations
★ Dallas
11551 Forest Central Drive, Ste. 300
Dallas, TX 75243
★ Houston
12929 Gulf Freeway, Ste. 111
Houston, TX 77034