Premature Rupture of Membranes
What is Premature Rupture of Membranes (PROM)?
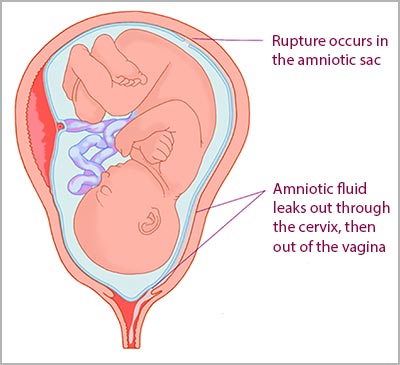
Premature rupture of membranes (PROM) is a medical condition that occurs after 37 weeks of gestation and before labor begins, when the amniotic sac holding the amniotic fluid and the baby ruptures. Commonly known as “water breaking,” rupture of membranes (ROM) usually prompts the onset of labor.
When PROM occurs before 37 weeks of pregnancy, it is termed as PPROM or preterm premature rupture of members. When ROM occurs along with or after the onset of labor prior to 37 weeks, it is termed as SPROM or spontaneous preterm rupture of membranes. When ROM at any stage persists for longer than 24 hours before the onset of labor, it is termed as prolonged ROM.
In most cases, PROM requires medical intervention and fetal heart rate monitoring. Loss of the protective amniotic sac layer puts the baby at an increased risk of birth complications, such as infections like Group B strep, umbilical cord compression/umbilical cord prolapse or breathing difficulties as a result of prematurity.
If these birth complications are not addressed and either prevented or timely treated, a baby could suffer a brain injury including hypoxic-ischemic encephalopathy (HIE) which can lead to cerebral palsy, neonatal encephalopathy (associated with multi-organ dysfunction), PVL or periventricular leukomalacia (white matter damage in the brain).
PROM occurs in approximately 8% of pregnancies. The earlier the water breaks, the greater are the health risks for the mother and the baby. An emergency cesarean section is usually advised in cases of PROM and PPROM.
What are the Causes and Risk Factors of PROM?
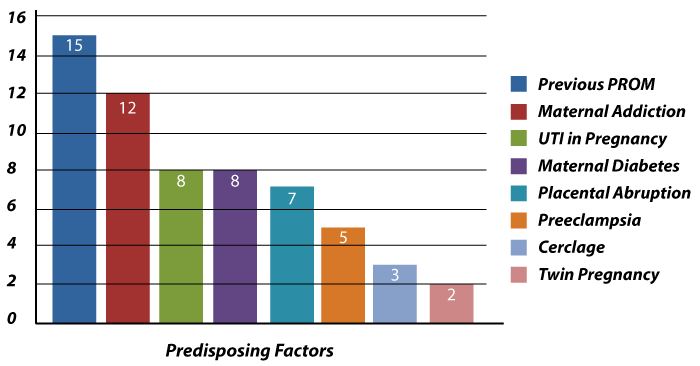
At full-term the water breaking (rupture of the membranes) is a normal part of labor and delivery. The science behind membrane rupture is as the mother labors or prepares to labor the activation of enzymes, programmed cell death and mechanical forces trigger the rupture of membranes. According to researchers, PROM probably occurs because of these same mechanisms and pathways, but with their premature activation. Risk factors of PROM may include:
- History of PROM in a previous pregnancy
- Placental abruption (separation of placenta from the inner uterine walls prior to birth)
- Intra-amniotic infection, such as chorioamnionitis
- Multiple pregnancy (twin pregnancy)
- Placenta previa, marked by antepartum vaginal bleeding
- Preterm labor
- Collagen vascular disorders
- Anemia
- Uterine septum or other uterus anomalies
- Excessive myometrial thinning (myometrium is the thick middle muscle layer of the fundus, which stretches in pregnancy to hold the growing baby)
- Cervical shortening (incompetent cervix) in the second trimester
- Advanced cervical dilation
- Polyhydramnios (excessive amniotic fluid)
- Oligohydramnios (insufficient amniotic fluid)
- Prior cervical conization (procedure to remove abnormal tissue from the cervix)
- Invasive uterine procedures (such as cervical cerclage, amniocentesis, or fetoscopy) during pregnancy, which may damage the membranes
- Chronic steroid therapy
- Multiple manual vaginal exams
- Nutritional deficiency (especially ascorbic acid and copper)
- Low BMI (body mass index)
- Substance use (such as cocaine)
- Cigarette smoking
- Direct abdominal trauma
How are Birth Injuries and Complications Associated with Premature Rupture of Membranes (PROM)?
Premature rupture of membranes (PROM) can cause fetal distress and other birth complications because the fetus is without the protective layer of amniotic fluid. Most of these birth complications may lead to cerebral palsy in babies if not diagnosed and treated appropriately. With vigilant fetal heart rate monitoring, ultrasound exams, blood tests, proactive administration of antibiotics and imaging tests, obstetricians and labor and delivery nurses can detect fetal distress early and perform a timely cesarean section to minimize the risk of complications.
Premature Birth
In the US, about 11% of all babies are born prematurely. PROM is the underlying cause of about 3 to 4% of these premature births. Preterm birth can contribute to various secondary birth complications, such as hypoxia or birth asphyxia, which may eventually lead to cerebral palsy.
When PROM occurs with a preterm baby (before 37 weeks) one of the main considerations of the medical team must be whether or not the baby’s lungs are adequately developed for a safe delivery. This will usually depend upon how premature the baby is when the premature rupture of the membranes occurs. Doctor and nurses have antenatal steroids, such as dexamethasone and betamethasone that can be given to the mother so her baby’s lungs develop more quickly when PROM occurs.
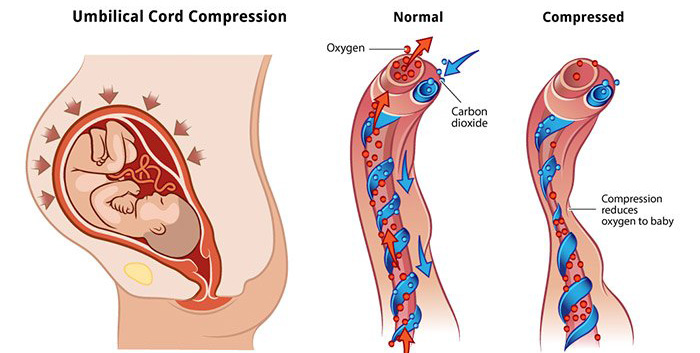
Prolapsed Umbilical Cord and Umbilical Cord Compression
PROM is one of the common causes of umbilical cord prolapse. In this condition, the cord slips into the birth canal before the baby’s descent. Umbilical cord compression can then occur if the baby gets trapped against the cord as they descend into the birth canal. This umbilical cord compression can reduce or even cut off the baby’s oxygen flow, posing the risk of hypoxic-ischemic encephalopathy (HIE), which may lead to cerebral palsy.
Maternal Infections
Infection is one of the most common complications associated with PROM for the baby and the mother. The amniotic fluid following PROM is exposed to any infection that the mother has because the protective barrier of the membranes has been lost. As a result the risk of infections, such as Group B Streptococcus, chorioamnionitis, bacterial vaginosis, urinary tract infection (UTI), and herpes simplex virus (HSV).
Obstetricians and nurses should almost always administer antibiotics when the premature rupture of the membranes occur to prevent any known or even unknown infection from occurring.
Malpresentation causing a Breech Delivery
PROM often results in a change of the fetal position and presentation. For instance, breech presentation can occur where the baby’s feet or buttocks or both move to so that they are positioned to come out first during birth. This may prompt the use of delivery assistance devices (such as forceps and vacuum extractors), increasing the baby’s risk of birth injury. When a breech baby is suspected after a PROM, the medical providers must be prepared to perform an emergency c-section if there is prolonged or arrested labor or if the electronic fetal monitoring strips show continuing fetal distress is occurring.
Respiratory Distress Syndrome
Following PPROM (preterm PROM), about 10 to 40% of the babies will develop respiratory distress syndrome (RDS). This acute morbidity occurs because the baby’s lungs are under-developed (pulmonary hypoplasia) and may not produce sufficient surfactant to keep them from collapsing. RDS can cause oxygen deprivation in the brain, increasing the baby’s risk of cardiac complications, HIE, and cerebral palsy.
Necrotizing Enterocolitis (NEC)
PROM is a risk factor for necrotizing enterocolitis (NEC), which is a severe gastrointestinal complication affecting many preterm babies. The intestinal tissue becomes inflamed in NEC and begins to die. Intestinal strictures (narrowing of the intestines) or abdominal infections due to perforations in the intestine are potentially life-threatening consequences of NEC.
Connection between PROM and Cerebral Palsy

Researchers conducted a retrospective cohort study of pregnancies complicated by PPROM (preterm PROM) and SPROM (spontaneous PROM) with delivery before 34 weeks of gestation. The study cohort consisted of 168 babies who underwent neurologic follow-up. The researchers identified 26 cases of cerebral palsy.
Factors related to cerebral palsy were identified as:
- Lower gestational age at PROM
- Longer latency (interval between PROM and labor)
- Chorioamnionitis related inflammation of the umbilical cord tissue
Researchers concluded that gestational age in PPROM and SPROM is significantly associated with cerebral palsy. The moment the rupture of membranes occurs in preterm PROM and spontaneous PROM, a process leading to brain damage may get triggered, which eventually causes cerebral palsy. As a result, doctors and nurses must be very aggressive in providing care and treatment to minimize the birth complications that can cause cerebral palsy following a preterm PROM.
How is a Diagnosis of Premature Rupture of the Membranes (PROM) made?
PROM and PPROM are primarily a clinical diagnosis. When an expectant mother reports watery vaginal discharge or leaking, the medical provider should confirm it with a sterile speculum exam (speculum is a device to look inside the vagina to observe the cervix). This minimally invasive diagnosis relies on the medical provider’s ability to determine three clinical signs on speculum examination:
- Fluid leakage from the cervical os (opening to the uterus) or visible pooling of fluid in the posterior fornix (larger recess behind the cervix)
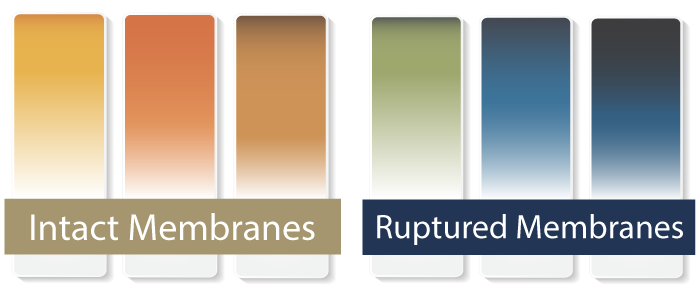
- Nitrazine test (which is a lab test) to detect the alkaline pH balance of the cervico-vaginal discharge (confirmed if the fluid turns nitrazine paper from yellow to blue)
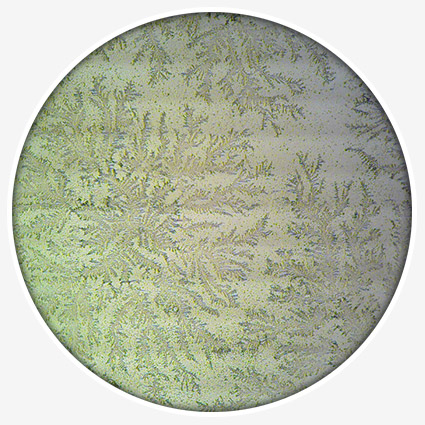
- Fern test to microscopically examine the cervico-vaginal discharge on drying to identify a “fern-like” pattern, indicative of PROM.
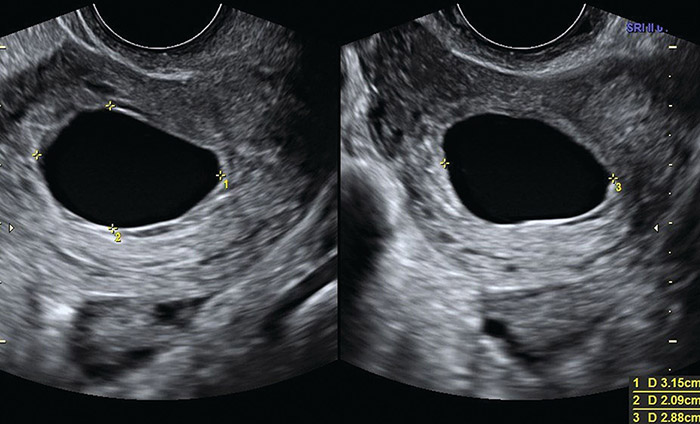
An ultrasound may also be used to detect evidence of oligohydramnios (low amniotic fluid volume). This alone will not confirm a PROM diagnosis, but may be used as supportive evidence to indicate it in a clinical setting.
What is the Significance of Early and Accurate PROM Diagnosis?
Accurate and timely preterm PROM diagnosis enables the medical team to make obstetric interventions appropriate to the gestational age of the baby. This can minimize the risk of severe complications, such as infections (neonatal sepsis or chorioamnionitis) and umbilical cord prolapse, while optimizing the perinatal outcomes.
How does Gestational Age matter once PROM has been diagnosed?
Doctors and nurses will manage the baby and expectant mother differently based upon the gestational age of the baby. This is primarily based upon the baby’s lung maturity at various stages of development. The closer to term, the more likely the baby’s lungs are going to be developed allowing a quicker delivery from time of PROM.
37 Weeks or Later
When PROM is diagnosed at 37 weeks of gestation or later, continuous fetal heart rate monitoring should be performed. Induction of labor methods (such as Pitocin infusion) should be commenced, or a cesarean section should be performed if it was planned. In case of Pitocin, the medical team should be prepared for a prolonged latent period of cervical dilation.
An emergency c-section should be performed if signs of fetal distress are detected during the monitoring. Antibiotic prophylaxis for Group B Streptococcus (GBS) should be administered when PROM lasts for more than 18 to 24 hours (regardless of the clinical GBS status).
34 to 36 Weeks
When a diagnosis of preterm PROM is made at 34 to 36 weeks of gestation, the medical team should be prepared to perform an emergency cesarean section or use labor induction methods (vaginal delivery is not contraindicated with preterm PROM).
The goal should be to avoid prolonging the pregnancy. Studies have shown that conservative PROM management at this stage increases the risk of complications. Corticosteroids for speeding up the maturity of the lungs are contraindicated at this stage, but the medical provider should prescribe antibiotics as a precaution (“prophylactically”) to eliminate the risk of maternal infections, such as Group B Streptococcus.
32 to 33 Weeks
When preterm PROM is diagnosed at 32 to 33 weeks of gestation, prolonging pregnancy should be avoided if the baby’s pulmonary maturity (lung development) is documented. Conservative management to prolong pregnancy in this situation unnecessarily increases the risk of umbilical cord compression, maternal amnionitis, and neonatal infection.
Medical providers should carefully weigh the risk of respiratory distress syndrome (RDS) associated with premature delivery against the risks of cord accidents and neonatal sepsis, which are associated with pregnancy prolongation in this condition. Antibiotics and corticosteroids should be administered and a cesarean section within 48 hours or at 34 weeks should be considered in consultation with a PPROM specialist and a neonatologist.
24 to 31 Weeks
At this stage, the goal of the medical provider should be to try and prolong the pregnancy up to 34 weeks. At the same time, the medical team should inform the patient and her caregivers that some patients may deliver within 7 days of preterm PROM.
Continuous fetal heart rate monitoring and other forms of fetal surveillance, such as biophysical profile and non-stress testing should be performed when preterm PROM is diagnosed before 32 weeks of gestation Delaying labor should be discontinued if non-reassuring fetal heart rate patterns (fetal distress) are observed in electronic fetal monitoring, or placental abruption, chorioamnionitis or other complications has occurred.
A Multi-Disciplinary Team Approach can Improve Outcomes
Immediate medical attention is vital when premature rupture of membranes occurs. Correct assessment of gestational age and accurate diagnosis are critical for appropriate patient management. The expectant mother should be carefully monitored for signs of infection. Continuous fetal heart rate monitoring should be performed to identify signs of fetal distress.
A team approach is always helpful and necessary to improve outcomes. The obstetrician should dictate patient management, a nurse should monitor the mother and the baby, and a pediatric team should be informed about the patient status so that they can prepare for the baby’s delivery. The anesthesia team should be informed in case obstetric anesthesia or a cesarean section is required.
Is Your Child’s PROM Related Birth Injury or Complication the Result of Medical Malpractice?
Parents whose children suffer from PROM related birth injury or complications want and deserve answers as to the cause of their child’s injury and whether mistakes by the doctors and nurses contributed to the injury.
- Were there signs of premature rupture of membranes during the pregnancy, or presence of risk factors such as a history of PROM, maternal infection, or vaginal bleeding which were either not recognized or properly treated?
- Did the medical team fail to provide precautionary antibiotics after premature rupture of the membranes occurred?
- Did an umbilical cord prolapse occur that was preventable or did the doctors and nurses fail to react to the prolapse in a timely manner?
- Was the decision to perform a cesarean delivery delayed despite the known birth complications due to PROM were occurring?
- During the labor and delivery, were there clear indications that the baby was suffering from fetal distress, but appropriate actions were not taken by the obstetrician or nurses?
- Did the neonatal resuscitation team delay in providing critical breathing support after birth?
- Were serious neonatal conditions like fetal hypoxia, hypoglycemia, or jaundice missed or treated incorrectly?
The experienced birth injury lawyers at Miller Weisbrod Olesky will help you determine if mistakes of the medical providers caused a birth injury to your child, including Hypoxic-Ischemic Encephalopathy (HIE) or cerebral palsy. Our hard working and successful birth injury attorneys have represented families all over the United States in their time of need after a birth injury. We use our experience and expertise to obtain for you and your child a medical malpractice settlement that will help provide specialized medical therapy in order to maximize the quality of life and independence of your child throughout their life.
Sometimes families are reluctant to contact a medical malpractice lawyer. It’s also not uncommon for parents to feel overwhelmed by the responsibilities they encounter in caring for their injured child and worried that they will not be able to help out in a lawsuit involving their child’s birth injury or complication. Our birth injury attorneys and nursing staff will address these hesitations and concerns, so you can focus on your child and maximizing their care.
Registered Nurses and Nurse-Attorneys Are a Vital Part of Our Birth Injury Team…and Yours

Most birth injury law firms will employ one or two nurses to assist the review of cases and medical research. But Miller Weisbrod Olesky offers an unmatched number of nurses and nurse-attorney employees support to both the birth injury attorneys and our clients.
Our team of registered nursing staff and nurse-attorneys bring a deep level of medical and personal insight to every client’s case. Our nursing team includes both an experienced labor and delivery nurse as well as an ICU nurse. Working closely with the rest of the team, they investigate the reasons behind a birth injury and how medical professionals breached their standard of care.
Why Should You Talk with the Knowledgeable Attorneys at Miller Weisbrod Olesky?

The only way to find out if you have a birth injury case is to talk to a lawyer experienced in birth injury lawsuits. It’s not uncommon that a birth related complication results in a preventable birth injury, including cerebral palsy, but it takes a detailed expert review by a birth injury attorney of the medical records from your child’s birth to determine if the birth injury was the result of medical malpractice.
At Miller Weisbrod Olesky, a team of committed lawyers, nurses and paralegals uses our detailed medical negligence case review process to assess your child’s potential birth injury case. We start by learning more about you and your child and the status of meeting/missing developmental milestones. Then we gather medical records to determine what happened before, during, and after your delivery. We call in skilled medical experts who review your records and let us know if they think medical errors could have caused your child’s injuries.
If we feel medical negligence caused or contributed to your child’s injuries, we meet with you to discuss how you can receive compensation from the medical professionals who made the errors. Our birth injury attorneys have recovered millions of dollars in settlements for families of children that have suffered a birth injury.
At no point in our legal intake process will we ask you to pay anything. The medical review of your case and the consultation are free. We only receive payment when you do.
Contact Our National Birth Injury Lawyers
National Birth Injury Law
Our National Birth Injury Attorneys, nurses, and support staff understand that parents of children with birth injuries feel overwhelmed. So, every client has the attention and support of a team of trained, compassionate professionals. But we don’t just offer compassion.
We offer a process to help you discover whether your child’s birth injury, HIE, cerebral palsy or brain injury at birth was caused by medical malpractice.
Call our offices today at (888) 987-0005 for experienced assistance in a free consultation.
Quick Links
Testimonials
- Lyric C. I feel like our voice was heard in a sense of what can possibly go wrong in a delivery and finding us answers. I feel with our settlement, we are now in a comfortable position to provide for our son.
- Lyssa L. They are not just people that say “hey let's get you money and let's go” The law firm was very thorough with us. It was awesome. I don't want to cry, because I think about and it's amazing that they were able to help me and that we were able to help my son and get the story out there.
- Jay C. Throughout the process, one thing was clear to us, the ultimate interest of our child was the utmost concern of Max and his team and as parents navigating a situation like that, that was refreshing to know we had them firmly on our side. I highly recommend them.
Popular Cities
- ★ Dallas Birth Injury
- ★ Houston Birth Injury
- ★ Atlanta Birth Injury
- ★ Chicago Birth Injury
- ★ Philadelphia Birth Injury
Locations
★ Dallas
11551 Forest Central Drive, Ste. 300
Dallas, TX 75243
★ Houston
12929 Gulf Freeway, Ste. 111
Houston, TX 77034